
KOLKATA, India — At the Seventy-ninth World Health Assembly (WHA79) in Geneva, Switzerland, on June 12, 2026, a powerful coalition of health ministers, policymakers, and global health advocates issued an urgent directive: political promises must immediately transition into hard infrastructure. Co-organized by South Africa and Nepal, the official side event, “Cervical cancer elimination: Strengthening health systems and accountability toward the 2030 targets,” marked a pivotal moment in the global campaign to dismantle a disease that claims hundreds of thousands of lives annually. The consensus was clear: the tools to eradicate cervical cancer exist, but failing healthcare delivery systems are keeping them out of reach for the world’s most vulnerable women.
The Stark Reality of a Preventable Killer
Cervical cancer occupies a unique and tragic position in modern medicine. It is highly preventable and entirely treatable if caught early, yet it remains one of the leading causes of cancer-related deaths among women worldwide.
According to data from the World Health Organization (WHO) and the International Agency for Research on Cancer (IARC), approximately 660,000 new cases were diagnosed globally in 2022, resulting in roughly 350,000 deaths. The geographic distribution of this crisis reveals a profound global health inequity. An overwhelming 94% of these fatalities occur in low- and middle-income countries (LMICs).
To put this into perspective: every two minutes, a woman dies from cervical cancer. In resource-constrained nations, less than 5% of women undergo regular screening. This failure stems from systemic bottlenecks, including prohibitive costs, logistically inaccessible clinics, and a critical shortage of trained pathology staff.
Addressing the Geneva assembly, H.E. Dr. Motsoaledi, Minister of Health of South Africa, emphasized that the obstacle is no longer medical ignorance, but operational execution.
“The science is established, the tools exist, and the strategies are in place,” Dr. Motsoaledi stated bluntly. “Progress now demands accountability.”
The 90-70-90 Framework
To systematically dismantle this crisis, 194 countries previously committed to the WHO’s Global Strategy to Accelerate the Elimination of Cervical Cancer. This strategy relies on hitting three interconnected public health benchmarks by the year 2030, known collectively as the 90-70-90 targets.
| Target | Core Strategic Goal | Public Health Impact (By 2120) |
| 90% Vaccination | Fully vaccinate 90% of girls with the Human Papillomavirus (HPV) vaccine by age 15. | 74 Million+ cases averted in low- and lower-middle-income countries. |
| 70% Screening | Ensure 70% of women are screened using a high-performance HPV test at age 35, and again by age 45. | 42% Reduction in median cancer incidence rates by 2045. |
| 90% Treatment | Successfully treat 90% of women identified with cervical disease (including pre-cancerous lesions and invasive cancer). | 97% Reduction in median cancer incidence rates, effectively eliminating the disease. |
The Human Cost of Fragmented Care
When these individual pillars operate in isolation rather than as a continuous chain of care, patients face devastating outcomes. This vulnerability was highlighted by Sally Kwenda, a cervical cancer survivor and prominent patient advocate who spoke at the event.
Kwenda’s testimony highlighted the dangerous gaps that persist between initial screening, diagnosis, and actual treatment, particularly for women navigating overlapping health crises. Women living with HIV, for example, face a six-fold higher risk of developing cervical cancer compared to women without HIV, making integrated clinical services a matter of survival.
“People are not diseases,” Kwenda reminded the assembly, calling for unified, person-centered care models that address a patient’s health needs under one roof.
Dr. Motsoaledi echoed this sentiment, noting that public health metrics must never obscure individual human lives: “None of this is abstract. Behind every percentage is a woman who either received care in time or did not.”
Country Realities: Local Innovations and Systemic Gaps
Reports shared by participating nations highlighted a mix of localized successes and steep, systemic hurdles:
-
Nepal’s Community Outreach: Health Minister Ms. Mehta detailed how Nepal leveraged its network of over 52,000 female community health volunteers to bridge “last-mile” gaps. This network deployed community-based HPV vaccinations, point-of-care “screen-and-treat” clinics, and pilot programs for at-home self-sampling.
-
Brazil’s Structured Implementation: Brazil reported strong vaccination gains by embedding HPV immunizations into public schools and funding targeted mobile health clinics for remote Amazonian and Indigenous communities.
-
Ghana’s Infrastructure Bottlenecks: Representatives from Ghana highlighted the challenges of integrating oncology services into primary healthcare. The country continues to face severe shortages in molecular diagnostic equipment, oncology nursing staff, and sustainable public financing.
-
Liberia’s Clinical Dilemma: Officials from Liberia illustrated a critical disconnect in care. While the country successfully trained more than 1,000 frontline health workers to perform visual screening using acetic acid (VIA), a profound lack of specialized surgical and radiation equipment means they frequently screen patients without any capacity to treat them.
Technological Innovations as Equalizers
To prevent clinical innovations from widening the gap between wealthy and developing nations, global health organizations emphasize that new technologies must be designed for rapid scaling.
“Innovation must translate into access at scale — not one without the other,” warned Mme Anne-Claire Amprou, Chair of the Unitaid Executive Board.
Single-Dose HPV Vaccines
One of the most significant clinical shifts occurred when the WHO updated its guidelines to endorse a single-dose HPV vaccine schedule based on robust trial data showing up to 98% protection against cervical cancer. By late 2024, 75 countries had transitioned to this single-dose regimen. This shift effectively halves procurement costs, simplifies school-based delivery logistics, and eliminates the steep patient drop-off rates associated with multi-dose schedules.
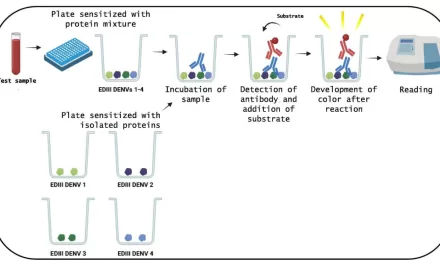
At-Home Self-Sampling
To bypass the stigma and logisitical barriers of traditional pelvic exams, high-performance HPV DNA self-sampling has emerged as a validated clinical alternative. These kits allow women to collect their own samples in privacy. Recognizing the utility of this approach, health agencies globally have updated their guidelines—including the U.S. Health Resources and Services Administration (HRSA) in early 2026—to formally include self-collection as a primary screening option for average-risk women.
The Vaccination Inequity and Pandemic Aftershocks
Despite clear medical consensus, vaccine distribution remains highly unequal. Data from Gavi, the Vaccine Alliance, reveals that while 98% of high-income countries have successfully integrated the HPV vaccine into their national immunization schedules, only 46% of low-income countries have done the same.
Global HPV Vaccination Status (Pre- vs. Post-Pandemic Impact)
────────────────────────────────────────────────────────────────────────
Pre-Pandemic (2010-2019 LMIC Average): ███████████████ 65% Coverage
Pandemic Disruption (2020-2021 Drop): ██████████ 50% Coverage
Recovery Target (Global 2030 Goal): ████████████████████ 90% Target
────────────────────────────────────────────────────────────────────────
The COVID-19 pandemic severely disrupted routine immunizations, driving average HPV vaccine coverage across LMICs down from 65% to 50%. While certain regions have shown remarkable resilience—notably Africa, where first-dose coverage climbed to 44% by the end of 2024—the lingering gaps mean an entire cohort of young girls remains unprotected as they approach adulthood.
Navigating the Path to 2030
Public health experts not involved in the direct WHA proceedings note that achieving a cervical cancer-free world requires acknowledging deep structural limitations. Building laboratory pipelines for HPV DNA testing, securing cold-chain refrigeration for vaccines, and retaining specialized medical personnel require long-term financial commitments that many developing nations cannot sustain alone.
Furthermore, screening campaigns that lack dependable treatment networks create a difficult ethical and clinical dilemma for local healthcare providers.
Dr. Tedros Adhanom Ghebreyesus, WHO Director-General, stressed that global equity must remain the operational standard rather than a secondary goal. “Every girl who remains unvaccinated and every woman who lacks access to screening or treatment is a reminder that equity must be at the heart of our elimination strategy,” Dr. Tedros stated.
For women globally, particularly across India and similar healthcare landscapes, these shifting policies emphasize a clear set of preventative actions:
-
Prioritize Early Immunization: Ensuring adolescent girls receive the HPV vaccine before age 15 provides highly effective, long-term protection against the primary viral strains that cause cervical malignancies.
-
Insist on High-Performance Screening: Standard Pap smears are increasingly being replaced by highly sensitive HPV DNA tests. Women should seek screening at age 35 and again at 45.
-
Utilize Modern Testing Alternatives: Where local cultural stigmas or clinic shortages limit access to speculum-based exams, women should inquire about validated self-sampling kits.
-
Demand Continuous Care: A screening result is only useful if backed by a clear clinical path. Patients must ensure their screening provider has an established referral network for immediate treatment if cellular changes are detected.
As the 2030 deadline approaches, the distinction between failure and success rests entirely on whether governments choose to fund and build accountable, integrated health systems. “At its heart, this movement is about justice,” concluded Dr. Saia Ma’u Piukala, WHO Regional Director for the Western Pacific. “It’s about ensuring that every girl and every woman, regardless of where she lives or what she earns, has access to basic, lifesaving care.”
Medical Disclaimer
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.










{kind=link}