

WASHINGTON — The White House on June 24, 2026, announced it will ask Congress for more than $1.4 billion in emergency supplemental funding to combat an expanding Ebola virus outbreak in Central Africa. Embedded within a broader $87.6 billion federal spending package, the newly proposed health funding is strictly earmarked for immediate international humanitarian relief, the construction of an American quarantine facility in Kenya, reinforced laboratory diagnostics, global disease surveillance, and diplomatic resources to manage high-risk medical evacuations. Public health officials framed the multi-pronged strategy as both an urgent humanitarian mission and a necessary defensive shield to keep the deadly virus from reaching United States shores.
Tracking the Expansion: The Bundibugyo Strain
The current crisis is unfolding across Central Africa, centered primarily within the Democratic Republic of the Congo (DRC) and Uganda. According to data released by the World Health Organization (WHO), this specific outbreak is driven by the Bundibugyo strain of the Ebola virus, a rarer variant than the heavily researched Zaire ebolavirus.
The epidemic has generated the largest number of confirmed cases within the first month of any recorded Ebola event. In its initial weeks, the virus has infected more than 1,000 individuals and claimed at least 267 lives, presenting distinct clinical and epidemiological challenges for global response teams.
Unlike the Zaire strain, which benefits from established, highly effective vaccines (such as Ervebo), the Bundibugyo strain lacks widely deployed, commercially standardized vaccines and targeted therapeutics. This makes traditional containment protocols—such as aggressive contact tracing, strict biological isolation, and early supportive clinical care—the primary lines of defense. The urgency of global containment was underscored this week when a humanitarian doctor returning to France from the DRC tested positive for Ebola, marking Western Europe’s first confirmed cross-border case linked to this outbreak.
+-------------------------------------------------------------------------+
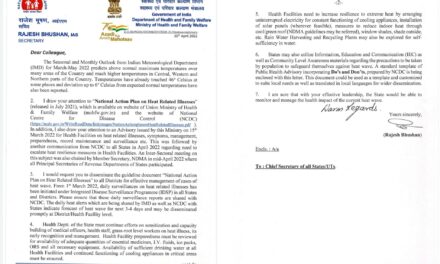
| THE $1.4 BILLION EBOLA FUNDING REQUEST |
+------------------------------------+------------------------------------+
| Humanitarian Crisis Response | $800 Million |
| Global Health Security Measures | $550 Million |
| Diplomatic & Evacuation Services | $90 Million |
+------------------------------------+------------------------------------+
Breaking Down the $1.4 Billion Emergency Budget
The White House’s formal fiscal request segments the emergency resources into three primary financial pillars, each addressing a separate point of vulnerability in the international response network.
1. International Humanitarian Assistance ($800 Million)
The largest portion of the funding is directed to on-the-ground crisis management in Africa. These funds are designed to supply front-line healthcare infrastructure with essential tools, including:
-
Personal protective equipment (PPE) and rapid infection-control training for local clinical staff.
-
The mobilization of mobile contact-tracing teams to trace and isolate transmission chains.
-
The establishment of a dedicated biological isolation and quarantine facility in Kenya, structured specifically to evaluate and isolate U.S. citizens and response workers who experience high-risk exposures.
2. Global Health Security ($550 Million)
Administered through Global Health Programs, this sector focuses on proactive biological containment. The funding aims to upgrade regional laboratory capacities in vulnerable nations bordering the outbreak zone to ensure local technicians can rapidly differentiate Ebola from endemic tropical fevers. Additionally, these resources will fund cross-border tracking networks and foster strategic public-private partnerships to fast-track regional diagnostics.
3. Diplomatic and Consular Emergencies ($90 Million)
Managed by the U.S. Department of State, this funding guarantees the logistics for secure medical evacuations. It provides the specialized containment transport, specialized aircraft, and diplomatic clearances necessary to airlift infected U.S. government personnel, researchers, or aid workers out of active hot zones and deliver them safely to high-consequence pathogen treatment centers within the United States.
Expert Perspectives: Quick Response vs. Systemic Fragility
Independent public health authorities broadly endorse the administration’s swift financial move, emphasizing that the economic and human cost of containing an outbreak multiplies exponentially the longer action is delayed.
Data compiled by global health research organizations, such as the Kaiser Family Foundation (KFF), demonstrates that emergency investments in localized disease monitoring drastically reduce the “spillover” potential—the risk of a pathogen successfully leaping onto international commercial flight networks and sparking domestic clusters.
However, some global health policy analysts caution that emergency supplemental funding acts as a temporary bandage rather than a permanent cure. Critics point out that prior to this sudden crisis, Washington faced persistent pushback for reducing its baseline, predictable funding to the U.S. Agency for International Development (USAID) and various African public health initiatives.
Experts note that relying on unpredictable emergency injections can disrupt steady, long-term health system stabilization in developing nations, leaving them repeatedly vulnerable when new biological threats emerge.
What This Means for Public Health and Daily Life
For the average citizen, health consumer, and traveler, the expanding outbreak and the subsequent White House funding request carry highly specific practical implications:
-
For Communities in Central Africa: If Congress authorizes and distributes these funds swiftly, local populations will see an immediate influx of treatment beds, safer clinical facilities, and improved access to supportive therapies, which significantly lowers Ebola’s historically high mortality rate.
-
For International Travelers: The risk to casual domestic travelers within the United States remains exceedingly low. However, the U.S. Centers for Disease Control and Prevention (CDC) and international partners have instituted strict travel parameters. Non-U.S. citizens who have recently traveled through the DRC, Uganda, or South Sudan are currently banned from entry, a restriction recently extended to green card holders who visited those nations within a 21-day window. Travelers heading to neighboring African aviation hubs should closely monitor official travel advisories, avoid informal clinical settings in affected areas, and practice meticulous hand hygiene.
-
For Domestic Healthcare Systems: Enhanced global monitoring acts as an early-warning radar system. By catching and containing cases at their source, domestic hospitals gain crucial lead time to review isolation protocols and train staff, ensuring the domestic frontline is prepared without causing unnecessary public alarm.
Legislative Hurdles and Structural Limitations
It is vital to note that a White House supplemental request is an initial proposal, not an absolute guarantee of funding. The package must navigate a divided Congress. Congressional aides have already signaled that the request faces an uphill battle; several lawmakers—including some key Republicans—have expressed deep reservations about voting for a broader $87.6 billion emergency bill that tethers vital global health security funds to highly polarized expenditures, such as ongoing military operations and domestic agricultural subsidies.
Furthermore, the public health impact of these funds depends entirely on operational speed. If partisan gridlock delays authorization by weeks or months, the containment window in Central Africa could close, allowing the Bundibugyo strain to seed itself across larger, more densely populated urban transport hubs, ultimately forcing a far more costly and complicated global intervention.
Medical Disclaimer
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.
References
Study & Epidemiological Citations
-
World Health Organization (WHO). (June 2026). Biannual Field Report on Pathogen Surveillance: Central African Bundibugyo Outbreak Dynamics. WHO African Regional Office.
Government & Public Policy Statements
-
The White House. (June 24, 2026). Estimate #2 – FY 2026 Supplemental: Departments of Agriculture, Energy, Homeland Security, the Interior, Justice, Labor, State. Formal Letter to the Speaker of the House of Representatives. [White House Archive ID: 2026.06.24-Supplemental-Johnson]
-
Centers for Disease Control and Prevention (CDC). (May/June 2026). Emergency Travel Orders and Amended Isolation Protocols for Green Card Holders and Non-Citizens Arriving from High-Consequence Ebola Areas. U.S. Department of Health and Human Services.
Media & Global Health Tracking Sources
-
Reuters Health News. (June 24, 2026). Exclusive: Trump Seeks More Than $1.4 Billion in Emergency Ebola Funding from Congress. Reported by Trevor Hunnicutt and Julie Steenhuysen.












{kind=link}