

DHAKA, Bangladesh — A devastating measles outbreak fueled by systemic vaccination gaps has claimed the lives of 499 people across Bangladesh, following the deaths of 11 more children within the last 24 hours. Data released today by the Directorate General of Health Services (DGHS) confirms the latest fatalities occurred between 8:00 AM yesterday and 8:00 AM today, marking this as one of the deadliest public health crises the nation has faced in recent history. The rapid surge, which began in mid-March 2026, highlights the fragile nature of herd immunity and the catastrophic speed with which airborne pathogens can exploit disruptions in routine immunization infrastructure.
Key Findings: The Staggering Scale of the Crisis
Public health surveillance data paints a sobering picture of the epidemic’s velocity. Nearly 68,000 individuals have been infected nationwide, a figure that includes 59,279 suspected cases and 8,275 laboratory-confirmed infections. The surge has pushed Bangladesh’s medical infrastructure to its limits:
-
Hospitalizations: 46,407 patients have required inpatient hospital care due to acute symptoms or secondary complications.
-
Recoveries: 42,336 individuals have been successfully treated and discharged.
-
Mortality Rate: The overall case fatality rate is hovering around 0.71%. This encompasses 85 deaths from laboratory-confirmed measles and 414 fatalities attributed to clinical complications arising from suspected cases.
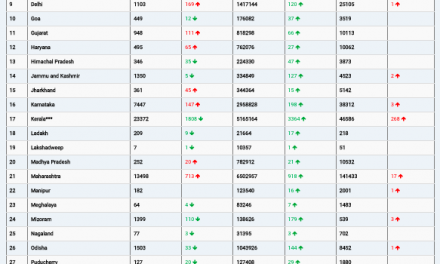
The geographic distribution shows that Dhaka Division is the primary epicenter, recording 28,599 suspected cases and 160 deaths. Conversely, Rajshahi Division has demonstrated a disproportionately high severity rate, logging 78 deaths despite documenting significantly fewer total cases.
Demographic analysis reveals that the youngest citizens are bearing the brunt of the crisis. Children under the age of five account for 82% of all documented infections. Alarmingly, nearly one-third of these affected children are infants under nine months of age—a cohort too young to receive the standard first dose of the measles vaccine under the routine national immunization schedule.
Expert Commentary: Understanding the Deadliness
International and local health authorities emphasize that the scale of this outbreak was entirely preventable. “Vaccines are foundational to child survival,” stated Rana Flowers, the UNICEF representative in Bangladesh. “The ongoing measles outbreak is placing thousands of children, particularly the youngest and most at risk, in grave danger.”
Dr. Halimur Rashid, Director of Communicable Disease Control at Bangladesh’s Health Department, noted that the volume of severe pediatric cases and fatalities has rapidly eclipsed historical trends. According to Dr. Rashid, the current crisis represents a stark, tragic reversal of decades of hard-won progress in national measles control.
Public health analysts argue that the biological virulence of the pathogen is only part of the problem. “Beyond immunization gaps, Bangladesh’s measles crisis reflects deep structural weaknesses,” explained Mohammad Mushtuq Husain, an adviser at the Institute of Epidemiology, Disease Control and Research (IEDCR) in Dhaka. He pointed out that when logistical chains break down, highly contagious viruses inevitably find and exploit the resulting pockets of unprotected populations.
Background: How Bangladesh Lost Its Shield Against Measles
The current epidemic stands in sharp contrast to Bangladesh’s historical success with immunization. Between 2014 and 2015, massive nationwide measles-rubella campaigns successfully vaccinated more than 50 million children. By the mid-2010s, the country maintained a first-dose coverage rate above 92%, while second-dose adherence exceeded 80%.
This protective shield began to erode due to a combination of global disruptions and domestic policy shifts:
-
The COVID-19 Pandemic: Beginning in 2020, critical resources and personnel were diverted to combat coronavirus. This mirrored a global trend noted by the World Health Organization (WHO), where suspended immunization programs left millions of children vulnerable.
-
Funding and Governance Shifts: Routine immunization lost priority under the interim government led by Muhammad Yunus. Believing that historically low measles rates implied long-term safety, officials halted certain vaccination funds. This administrative neglect was compounded by political instability throughout 2024.
-
Procurement Overhauls: In September 2025, the interim government discontinued its long-standing vaccine procurement program managed through UNICEF, opting instead for an open tender system. UNICEF strongly opposed this transition, warning that altering established supply chains could trigger catastrophic shortages.
By the time the outbreak manifested in March 2026, the consequences of these decisions became clear. Health Minister Sardar Md Sakhawat Hossain acknowledged that the current administration inherited “a complete shortage of measles vaccines, with not a single dose” left in the national stockpile.
Measles: Why This Virus Is So Dangerous
Measles is caused by the Measles morbillivirus, an apex airborne pathogen. It is so highly contagious that if an infected person enters a room, up to 9 out of 10 unvaccinated individuals in that vicinity will contract the virus.
While often perceived erroneously as a simple childhood rash, measles causes profound systemic immune suppression and severe clinical complications:
| Complication | Statistical Risk Level | Clinical Consequences |
| Pneumonia | 1 in 20 infected children | The most common cause of measles-related death in young children. |
| Encephalitis | 1 in 1,000 infected children | Brain swelling that can cause convulsions, permanent deafness, or intellectual disabilities. |
| Hospitalization | 1 in 5 unvaccinated people | Required due to severe dehydration, respiratory distress, or secondary infections. |
| Death | 1 to 3 in 1,000 children | Resulting primarily from severe respiratory and neurological destruction. |
Note: Children under five, adults over twenty, pregnant women, and individuals with compromised immune systems face the highest risk of experiencing these severe outcomes.
Emergency Vaccination Campaign Mobilized
In an effort to blunt the trajectory of the epidemic, the Ministry of Health has designated 30 high-incidence “hotspots” across 20 districts for emergency intervention. An emergency measles-rubella vaccination campaign was deployed on April 5, 2026.
The initiative initially targeted 1.2 million children aged 6 to 59 months. It has since expanded broadly into congested urban sectors, with major operations concluding this week. To date, approximately 17 million children have received emergency measles-rubella inoculations.
Special operational emphasis has been directed toward Dhaka, owing to its dense population dynamics, and Cox’s Bazar, which hosts sprawling, vulnerable Rohingya refugee camps. The WHO and international partners are providing technical support, reinforcing laboratory diagnostic capacity, and optimizing hospital case-management protocols to mitigate the mortality rate.
Limitations and Counterarguments: Why the Outbreak Persists
Despite the scale of the emergency response, several compounding factors prevent immediate containment:
-
Immunity Gaps: Multiple consecutive birth cohorts missed their routine vaccinations over the last few years, creating a vast reservoir of susceptible hosts.
-
Population Mobility: High-density travel during recent festive seasons acted as an epidemiological accelerator, carrying the virus from urban centers into rural communities.
-
Logistical Cascades: Ongoing vaccine procurement delays mean that local supply chains are still playing catch-up to the sheer speed of transmission.
-
Infant Vulnerability: Because standard schedules administer the first dose at nine months, the large cohort of infected infants under this age remains biologically unprotected.
Officials from the interim administration have defended the structural changes that precipitated the vaccine shortage. Sayedur Rahman, former vice chancellor of Bangladesh Medical University and a key health adviser to the interim government, argued that the previous UNICEF-reliant procurement system required alteration because it relied on legal clauses intended solely for temporary emergencies. Rahman stated the administration sought to establish a “regular, rule-based system going forward” to maximize fiscal transparency and eliminate perceptions of bias.
However, the human cost of this administrative transition has drawn sharp criticism. “Given the dramatic fallout, the decision to change the procurement system needs to be investigated,” countered UNICEF’s Rana Flowers, highlighting that policy transitions should never compromise active biosecurity shields.
Global Health Implications and Daily Prevention
The crisis in Bangladesh serves as a stark reminder to the global community of how quickly a forgotten disease can return. Measles remains a leading vaccine-preventable cause of death worldwide; according to WHO data, approximately 95,000 people—mostly young children—died from the disease globally in 2024 alone.
For health-conscious families and communities worldwide, the outbreak underscores several vital public health realities:
-
Herd Immunity is Essential: Maintaining a vaccination coverage rate of at least 95% is vital to establishing herd immunity. This high threshold is the only mechanism that shields vulnerable infants who are too young to be immunized.
-
Two Doses are Mandatory: A single dose of the measles-mumps-rubella (MMR) vaccine provides roughly 93% effectiveness. Completing the two-dose series elevates protection to approximately 97%.
-
Recognize Symptoms Early: Measles begins with a high fever, cough, coryza (runny nose), and conjunctivitis (watery, red eyes). The characteristic maculopapular rash emerges 7 to 14 days after initial exposure, spreading from the face downward.
The Path Forward
Bangladesh’s Health Minister has pledged to bring the outbreak under complete control within the calendar year, taking the emergency step of canceling leaves for medical personnel to ensure hospitals remain adequately staffed. The immediate focus remains on executing localized catch-up vaccination campaigns, rebuilding the shattered routine immunization infrastructure, and stabilizing national vaccine procurement pipelines.
The tragedy unfolding in Dhaka and surrounding divisions demonstrates that measles elimination is never a permanent victory. Preserving protection against highly contagious diseases demands unwavering political will, consistent funding, and resilient public health infrastructure—lessons that carry profound weight far beyond the borders of Bangladesh.
Medical Disclaimer
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.
References
Study and Data Sources
-
Directorate General of Health Services (DGHS), Bangladesh. Epidemiological monitoring report: “Measles Outbreak: 11 More Children Die, Death Toll Rises to 499.” Published May 22, 2026.











{kind=link}