
NEW DELHI — As 2026 unfolds, India finds itself at a critical crossroads in cardiovascular medicine. The nation’s catheterization labs have never been more advanced, boasting “smarter” drug-eluting stents and micron-level precision imaging that rival the best facilities in the world. Yet, beneath the shimmer of chrome and high-tech screens, a sobering reality persists: the heart disease epidemic is getting younger, more complex, and more lethal.
Leading cardiologists warn that while a stent can open a blocked artery in minutes, it cannot fix the systemic and behavioral issues that lead a patient to the operating table in the first place. As coronary artery disease (CAD) increasingly strikes Indians in their 30s and 40s, the medical community is shifting its focus from the “quick fix” of the procedure room to a more holistic, multidisciplinary approach to long-term survival.
A Crisis in the Youth: The Changing Face of CAD
The statistics painting India’s heart health landscape are startling. Cardiovascular disease (CVD) now accounts for nearly 25% of all deaths in the country. More concerning is the age at which these events occur. Research indicates that CAD strikes Indians roughly a decade earlier than Western populations, with more than half of CAD-related deaths occurring before age 50.
Recent clinical data suggests that one in five heart attack patients in India is now under the age of 40. This shift is driven by a “perfect storm” of rapid urbanization, sedentary lifestyles, and a genetic predisposition to metabolic conditions.
“We are seeing 30-year-olds with the coronary arteries of 70-year-olds,” says Dr. Sripal Bangalore, Professor of Medicine at New York University School of Medicine. “The complexity of the disease in younger Indians means we aren’t just treating a single blockage; we are managing a lifelong condition that started far too early.”
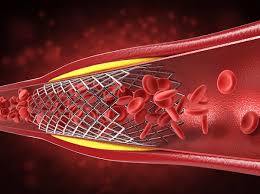
The Evolution of the Stent: From Scaffolds to Precision Tools
While the prevention side of the equation remains a challenge, the technology used to treat acute blockages has seen remarkable breakthroughs. Modern Drug-Eluting Stents (DES) have moved far beyond the rigid metal coils of the past.
According to Dr. Nils P. Johnson, Professor of Cardiology at the University of Texas, Houston, the latest generation of stents offers two primary advantages:
-
Engineering: Stents are now thinner and more flexible. This is crucial for the “tortuous” or highly curved anatomy often found in Indian patients, allowing the device to conform to the vessel without causing trauma.
-
Pharmacology: The coatings that release medication to prevent scar tissue regrowth are more biocompatible, allowing the artery to heal naturally while keeping the passage clear.
The Role of Precision Imaging
To complement these devices, cardiologists are increasingly using Optical Coherence Tomography (OCT). In a vessel only 3 to 5 millimeters wide, there is no room for error. OCT provides near-micron-level visualization from inside the artery, allowing doctors to ensure the stent is perfectly sized and pressed against the vessel wall. Studies have shown that imaging-guided stenting significantly lowers the risk of stent thrombosis (sudden clotting) and the need for repeat procedures.
The Hidden Enemy: Lipoprotein(a)
While high blood pressure and smoking remain top-tier risks, researchers are zeroing in on a non-traditional marker that is particularly prevalent in the Indian population: Lipoprotein(a), or Lp(a).
Lp(a) is a genetically determined, cholesterol-rich particle that promotes both plaque buildup and blood clotting. Unlike “bad” LDL cholesterol, Lp(a) levels are largely unaffected by diet or exercise.
-
The Indian Context: Approximately 25% of Indians have high Lp(a) levels ($\ge 50$ mg/dL).
-
The Risk: High Lp(a) confers a two- to three-fold higher risk of CAD, a threat level comparable to—or exceeding—diabetes in certain groups.
“Lp(a) is emerging as a key player among younger Indians with heart problems,” Dr. Bangalore notes. For many young patients who have no traditional risk factors like obesity or smoking but still suffer heart attacks, Lp(a) is often the “hidden” culprit.
Beyond the Procedure: The “Heart Team” and Patient Adherence
The most advanced stent in the world is only as effective as the care that follows it. Experts argue that India’s resource-constrained settings often see a “drop-off” in care once the patient leaves the hospital.
The Missing Link: Adherence
Real-world data shows that many Indian patients discontinue essential medications—such as anti-platelets and statins—within months of their procedure. This is often due to a lack of symptoms (“I feel fine now”), the cost of medication, or a misunderstanding of the chronic nature of the disease.
The “Heart Team” Model
To manage complex patients—those with diabetes, kidney disease, or multiple blockages—top Indian hospitals are adopting the “Heart Team” approach. This involves a collaborative group of interventional cardiologists, cardiac surgeons, and preventive specialists. Instead of a single doctor making a high-pressure call, the team weighs whether optimal medical therapy, stenting, or bypass surgery is the safest long-term path for the individual.
Practical Advice: What Should Patients Do?
For families concerned about heart health, the medical community offers a clear roadmap that emphasizes lifestyle over “mechanical fixes”:
-
Medication is Mandatory: Never stop prescribed heart medications without consulting your doctor. Even if you feel healthy, these drugs prevent the next event.
-
Screen Early: Don’t wait for chest pain. Screen for blood pressure, glucose, and lipids by age 25. If there is a family history of early heart attacks, request an Lp(a) test.
-
The 150-Minute Rule: Aim for at least 150 minutes of moderate-intensity exercise per week.
-
Dietary Shift: Prioritize whole grains, nuts, and vegetables while drastically reducing salt and refined carbohydrates.
Limitations and the Road Ahead
While technology has improved, it is not a silver bullet. Some experts caution that focusing too heavily on expensive devices without strengthening primary care and tobacco control may only shift the disease burden rather than reduce it.
Furthermore, while Lp(a) is a known risk factor, global clinical trials are still ongoing to determine if specifically lowering Lp(a) levels will reduce the actual number of heart attacks. Until then, aggressive management of all other modifiable risks remains the gold standard.
In the end, India’s path to a healthier heart lies not just in the hands of the surgeon, but in the daily choices of the patient and a healthcare system that values prevention as much as the procedure.
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.
References
- https://health.economictimes.indiatimes.com/news/industry/indias-heart-care-needs-more-than-cutting-edge-stents/130166044?utm_source=top_story&utm_medium=homepage












{kind=link}