
SHILLONG – Health authorities in Meghalaya have implemented an emergency surveillance net across the 443-km India-Bangladesh border following a surge in measles cases in the neighboring nation. With Bangladesh reporting over 18,000 suspected cases and dozens of fatalities since mid-March 2026, Meghalaya officials are mobilizing community health workers and border forces to prevent a cross-border spillover that could threaten vulnerable pediatric populations.
The intensified measures, announced on April 20, 2026, come as transmission has reached 58 of Bangladesh’s 64 districts. In response, the Meghalaya Health Department has directed schools, anganwadi centers, and Integrated Child Development Services (ICDS) to treat every instance of “fever with rash” as a suspected measles case, requiring immediate notification to the nearest medical officer.
The Crisis Next Door: Unpacking the Bangladesh Outbreak
The scale of the current outbreak in Bangladesh has caught regional health experts by surprise. According to data from the World Health Organization (WHO) and local health ministries, 18,219 suspected cases were logged between March 15 and April 14, 2026. Of these, 2,897 have been laboratory-confirmed.
The human toll is particularly heavy among the youngest citizens:
-
Case Fatality Rate (CFR): Currently sits at 1.2%, with 164 suspected deaths.
-
Demographics: Children under the age of five account for approximately 80% of all infections.
-
Geographic Intensity: The divisions of Dhaka and Barisal are currently the epicenters, with incidence rates soaring to 39.4 per million population.
Experts attribute this “explosion” of cases to a combination of factors, primarily a “immunity gap” left by declining routine immunization rates and vaccine supply disruptions in 2025.
Meghalaya’s “Proactive Defense” Strategy
Meghalaya’s response is focused on districts with high cross-border mobility, including East Khasi Hills, South West Garo Hills, and West Jaintia Hills. Unlike previous reactive measures, the current strategy emphasizes early isolation and community reporting.
“Suspected cases should remain isolated at home with minimal contact to prevent further transmission,” stated an official from the East Khasi Hills district. This isolation is critical because measles is one of the most contagious diseases known to science; a single infected person can infect up to 12 to 18 others in an unvaccinated population.
State authorities are coordinating with the Border Security Force (BSF) and WHO Rapid Response Teams to monitor transit points. Dr. B. Puspakarna, a member of the WHO team, has been briefing local stakeholders on the risks of aerosol transmission. While no confirmed cases linked to the current Bangladesh surge have been detected in Meghalaya yet, health officials point to the 2017 Jaintia Hills outbreak—which was fueled by low vaccination coverage—as a cautionary tale.
Understanding the Threat: Why Measles is Rising
Measles is caused by a highly contagious virus in the paramyxovirus family. It spreads through the air via respiratory droplets when an infected person coughs or sneezes.
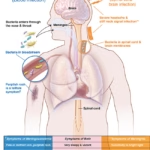
Symptoms and Progression
-
Incubation (7–14 days): No symptoms.
-
Prodromal Stage: High fever, cough, coryza (runny nose), and conjunctivitis (red, watery eyes).
-
Exanthem Stage: The characteristic red, blotchy rash appears, typically starting on the face and spreading downward to the body and limbs.
“Measles is not just a ‘childhood rash.’ It is a serious respiratory virus that can ‘reset’ the immune system, making children more vulnerable to other deadly diseases for months or even years,” explains Dr. K. Bagai, a physician monitoring regional infectious diseases.
The Vaccination Gap: A Fragile Shield
The primary driver of the current crisis is a failure to reach “herd immunity.” For measles, this requires a staggering 95% vaccination coverage with two doses of the Measles-Rubella (MR) vaccine.
While India’s national MR coverage is relatively strong—93.7% for the first dose and 92.2% for the second dose in 2024-25—pockets of “zero-dose” children remain in the northeastern states. These clusters represent the greatest risk for a localized outbreak if the virus crosses the border.
In contrast, Bangladesh’s health system has struggled with funding cuts and vaccine shortages. Dr. Benazir Ahmed, former Director of Disease Control in Bangladesh, noted that while the goal was elimination by 2026, the current struggle highlights the fragility of immunization infrastructure.
Guidance for the Public and Healthcare Providers
For residents in border districts and health-conscious citizens, the message from medical professionals is clear: Vaccination is the only effective defense.
For Parents and Caregivers:
-
Check Records: Ensure your child has received two doses of the MR vaccine (typically at 9-12 months and 16-24 months).
-
Monitor Symptoms: If a child develops a fever and a rash, isolate them immediately and contact a healthcare provider. Do not visit a crowded clinic without calling ahead, as the virus can linger in the air for up to two hours.
-
Supportive Care: There is no specific antiviral treatment for measles. WHO recommends two doses of Vitamin A supplements for children diagnosed with measles to help prevent eye damage and reduce the risk of death.
For Travelers:
-
Adults who are unsure of their vaccination status and plan to travel to high-risk divisions like Dhaka or Barisal should consult a doctor regarding a booster or evidence of immunity.
Public Health Outlook: A Race Against Time
The Bangladesh Ministry of Health, supported by UNICEF and Gavi, launched an emergency MR vaccination campaign on April 5, targeting 1.2 million children. The success of this campaign is vital not just for Bangladesh, but for the entire South-East Asian region.
While India remains in a stronger position due to high vaccination coverage, the movement of people across borders means no state is entirely immune. As Dr. Lalmuanawma Jongte, Senior Chief Medical Officer in Mizoram, noted: “Complacency is our biggest enemy. Vaccination remains the most effective safeguard we have against this preventable tragedy.”
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.
References
https://www.uniindia.com/meghalaya-health-authorities-intensify-preparedness-amid-measles-outbreak-in-bangladesh/east/news/3816866.html












{kind=link}