
LONDON — In a major shift in public health strategy, British vaccine advisers have recommended that the meningococcal B (MenB) vaccine be routinely offered to teenagers around the age of 15. The landmark recommendation, published on July 16, 2026, by the Joint Committee on Vaccination and Immunisation (JCVI), follows an unprecedented outbreak of the disease in Kent earlier this year and a thorough review of new clinical evidence regarding vaccine longevity, safety, and real-world performance. The proposal has now been submitted to the Department of Health and Social Care (DHSC) for ministerial review before any formal updates are integrated into the National Health Service (NHS) immunization schedule.
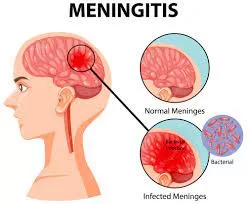
Meningococcal B is the leading cause of invasive meningococcal disease (IMD) in the UK. IMD is a rare but exceptionally severe bacterial infection that can rapidly progress to meningitis (inflammation of the protective membranes covering the brain and spinal cord) and septicemia (blood poisoning). The disease is notorious for its swift onset and devastating consequences, frequently resulting in lifelong neurological disabilities, limb amputations, or death within hours of the first symptoms. By targeting 15-year-olds, public health officials aim to fortify immunity during a developmental window when young people become more socially active, thereby facing a significantly elevated risk of bacterial transmission.
A Shift in Strategy: Who is Eligible?
The newly proposed framework introduces a tiered approach designed to maximize population immunity based on prior vaccination history:
-
Routine Single Dose: A single booster-like dose will be offered to young adolescents around age 15 who previously received the MenB vaccine during infancy.
-
Two-Dose Primary Regimen: A full two-dose series, administered at least 28 days apart, is strongly recommended for older adolescents who did not receive the vaccine as babies, as well as designated catch-up groups.
This strategy builds directly upon the UK’s existing immunization infrastructure. In 2015, the UK became the first country in the world to introduce the four-component serogroup B meningococcal vaccine (4CMenB), commercially known as Bexsero, into its routine infant national immunization program following a 2014 JCVI recommendation.
Data compiled by the UK Health Security Agency (UKHSA) confirms that the infant program remains highly effective, providing robust protection that lasts for at least five years. However, as the first cohort of vaccinated infants approaches their teenage years, immunologists note that natural antibody levels decline. The adolescent booster is strategically timed to bridge this emerging immunity gap before teenagers enter high-density living and social environments.
The Weight of the Evidence
The JCVI’s decision to alter its stance on adolescent vaccination follows an independent expert review initiated after a severe localized outbreak in March 2026. The committee’s comprehensive assessment synthesized real-world data tracking vaccine effectiveness, current meningococcal epidemiological trends, and shifting outbreak patterns across the UK.
Public health logic for school-age immunizations relies on preemptive defense: immunizing a population before their statistical risk spikes rather than reacting after widespread transmission has occurred. Teenagers and young adults are known asymptomatic carriers of Neisseria meningitidis bacteria in the back of their nose and throat. As adolescents transition into crowded environments—such as high schools, college dormitories, and university housing—close contact facilitates the exchange of respiratory and throat secretions, driving up infection rates.
Furthermore, the committee evaluated emerging data suggesting that the 4CMenB vaccine may offer additional cross-protection against gonococcal infections (gonorrhea), a sexually transmitted infection caused by a related bacterial species, Neisseria gonorrhoeae. This secondary benefit added weight to the overall public health utility of the adolescent program.
The clinical foundation of the vaccine itself is well-established. A seminal national observational cohort study published in The Lancet analyzed the initial roll-out of the 4CMenB vaccine in England. The study recorded a striking 50% reduction in MenB cases among vaccine-eligible infants within just 10 months of the program’s inception, concluding that even a reduced infant schedule yielded high real-world effectiveness. Additionally, a comprehensive 2023 review published in Human Vaccines & Immunotherapeutics evaluated extensive clinical and post-marketing surveillance data, reaffirming that the vaccine maintains a reassuring safety profile with mostly mild, transient side effects such as localized soreness or low-grade fever.
Expert Perspectives on Equity and Risk
Medical experts emphasize that while meningococcal disease is rare, its catastrophic impact justifies robust preventative measures.
“Invasive meningococcal disease is rare but very serious, and it can have a devastating impact on lives,” stated Professor Wei Shen Lim, KBE, Chair of the JCVI, noting that the committee heavily weighed the profound experiences of families affected by the illness when formulating the advice. Professor Lim also strongly urged currently eligible young people to utilize the existing one-off summer vaccination programs before departing for universities or colleges in the autumn.
In public health economics, expanding a vaccine program requires balancing financial cost against preventable disease burden. In this instance, the JCVI explicitly acknowledged that the long-term cost-effectiveness of a universal adolescent program remains mathematically uncertain. However, the committee ultimately supported the proposal on equity grounds, determining that implementing the adolescent program serves as a vital bridge to eliminate protection gaps until a permanent, routine framework can be fully integrated.
Commenting independently on the development, Dr. Helen Jenkins, a consultant in pediatric infectious diseases who was not involved in the JCVI review, praised the proactive nature of the advice.
“With meningococcal disease, you cannot afford to be reactive. The Kent outbreak demonstrated how quickly this pathogen can exploit pockets of low immunity in young people. Even when cost-effectiveness models show uncertainty, the human cost of managing severe disability or losing a teenager to a vaccine-preventable infection outweighs the ambiguity. Closing the immunity gap at age 15 is a highly logical step.”
Program Limitations and Uncertainties
Despite the strong backing from experts, several caveats remain. Because the JCVI functions as an advisory body, the recommendation is a formal proposal rather than finalized law. The implementation timeline depends entirely on ministerial approval and funding allocations from the Department of Health and Social Care.
Additionally, critics and epidemiologists point out that outbreak-driven policy shifts can be vulnerable to shifting local conditions. A vaccination strategy optimized in response to a severe regional spike, like the one witnessed in Kent, may display altered cost-benefit ratios if overall national disease levels naturally recede or if circulating bacterial strains mutate over time. Because no vaccine provides 100% absolute protection, continuous molecular surveillance of meningococcal strains remains critical to ensure the vaccine continues to match circulating bacteria.
What Consumers and Families Need to Know
For the general public, health officials emphasize that the primary takeaway should be heightened awareness rather than anxiety. The overall risk of contracting MenB remains low, but because the disease escalates with extreme velocity, recognizing the warning signs is lifesaving.
Early symptoms often mimic the flu, but individuals should seek emergency medical attention immediately if a teenager or young adult exhibits a combination of the following:
-
A sudden, high fever accompanied by severely cold hands and feet
-
An intense, debilitating headache or severe muscle pain
-
Projectile vomiting or a refusal to eat
-
A stiff neck or an extreme sensitivity to bright lights (photophobia)
-
Confusion, drowsiness, or difficulty waking up
-
A characteristic petechial rash (small red or purple spots that do not fade when firmly pressed with a clear glass)
For British families, immediate action centers on verifying eligibility. The routine 15-year-old offer will eventually target adolescents born on or after May 1, 2015. For older teenagers, a separate catch-up campaign is being structured. Notably, a one-off summer immunization program is actively available right now for eligible young people, particularly prospective students preparing to enter residential further education or university dormitories in autumn 2026.
Ultimately, this recommendation underscores a core tenet of modern immunology: vaccines are most effective when precisely timed to match periods of maximum exposure. By reinforcing defenses right as adolescents step into wider social circles, the proposed strategy seeks to ensure that the success of the UK’s infant vaccine program is carried safely into adulthood.
References
-
Reuters Health. (July 16, 2026). “UK experts recommend MenB vaccine for 15-year olds following big outbreak.”
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.












{kind=link}