

Published: June 29, 2026
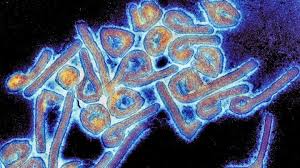
A growing body of landmark research has revealed that the Oropouche virus—an insect-borne pathogen historically believed to cause localized, self-limiting outbreaks—has quietly swept across Latin America and the Caribbean on a scale previously unimagined.
New mathematical modeling and serological analyses published in Nature Medicine and Nature Health estimate that approximately 9.4 million people have been infected with the virus since 1960. Brazil alone accounts for an estimated 5.5 million of these cases.
The findings expose massive gaps in global disease surveillance, proving that relying solely on confirmed clinical diagnoses leaves public health systems operating in a profound blind spot. Because Oropouche symptoms closely mimic those of dengue, millions of cases have been misdiagnosed, ignored, or caught too late, obscuring the true public health burden of the disease.
Unveiling the “Missing” Millions
For decades, official case registries painted Oropouche as a minor, regional concern confined to the Amazon basin. However, the new studies utilize a sophisticated combination of historical epidemiological data, mathematical transmission modeling, and blood-bank antibody testing to reconstruct the true footprint of the virus.
The disparity between documented cases and estimated infections is starkest in recent data. During the intense 2023–2024 outbreak, the city of Manaus—a major urban hub in the Brazilian Amazon—experienced what researchers estimate to be 300,000 infections. Routine clinical surveillance captured only a tiny fraction of this surge.
Estimated Oropouche Infections (1960–2026)
┌───────────────────────────────────────┬───────────────────────────────┐
│ Region │ Estimated Total Infections │
├───────────────────────────────────────┼───────────────────────────────┤
│ Latin America & Caribbean (Total) │ 9.4 Million │
│ Brazil │ 5.5 Million │
│ Manaus, Brazil (2023–2024 Outbreak) │ 300,000 │
└───────────────────────────────────────┴───────────────────────────────┘
To validate these modeling estimates, scientists analyzed anonymous blood-donor samples in Manaus to track the presence of Oropouche-specific antibodies. They discovered that antibody prevalence among the population skyrocketed from 11.4% in November 2023 to 25.7% by November 2024. This rapid doubling provides concrete biological evidence that the virus was spreading widely and silently through the community.
Why Oropouche Evaded the Diagnostic Radar
The primary driver behind this diagnostic erasure is symptom overlap. Oropouche virus disease typically presents with a sudden fever, severe headache, muscle aches, and joint pain—a clinical picture virtually identical to dengue, zika, and chikungunya, which are highly endemic to the same geographic regions.
“When two distinct infections look identical in a clinic, the official numbers reflect whatever disease healthcare providers are actively looking for,” explains an independent epidemiologist not involved in the studies. “In most rural or resource-limited clinics, if a patient tests negative for dengue, or if dengue tests are unavailable, the illness is simply chalked up to an unspecified viral syndrome. The patient goes home, recovers, and the data is lost forever.”
Furthermore, standard public health networks are inherently reactionary. They are designed to capture patients who are sick enough to seek hospital care, who present during the narrow window when molecular testing (like RT-PCR) is accurate, and who reside near laboratories equipped with specialized reagents. For a virus spread by Culicoides paraensis midges and certain mosquitoes, the vast majority of mild or moderate infections never trigger a laboratory test.
The World Health Organization (WHO) has long urged member states to diversify and strengthen their diagnostic toolkits for emerging pathogens. These new findings reinforce the WHO’s warnings, showing that without active surveillance, public health planning is forced to combat epidemics using outdated and incomplete maps.
Beyond the Fever: Severe Complications Re-evaluated
While most individuals recover from Oropouche without lasting illness, the sheer volume of hidden infections means that rare, severe complications are occurring far more frequently in absolute numbers than previously realized.
Data published in the recent studies indicates that approximately 1 in every 1,000 diagnosed cases may progress to severe clinical outcomes. Public health officials are particularly concerned by several emerging patterns of complications:
-
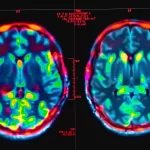
Neurological Invasions: The virus can cross the blood-brain barrier, leading to potentially life-threatening conditions such as meningitis and meningoencephalitis (inflammation of the brain and surrounding membranes).
-
Vertical Transmission: Evidence suggests the virus can pass from a pregnant person to the fetus, associated with miscarriages and congenital abnormalities such as microcephaly.
-
Organ Damage: A small percentage of severe cases exhibit acute liver complications.
“We must understand that a ‘small fraction’ of a massive number is still a large and dangerous burden on a healthcare system,” notes José Luiz Proença Módena, coordinator of the Laboratory for the Study of Emerging Viruses (LEVE) at the University of Campinas (UNICAMP), who contributed to the broader scientific discourse surrounding the virus. Módena emphasizes that the true magnitude of the disease requires heightened, immediate public health attention globally.
Clinical Realities and Public Health Action
For healthcare professionals, these insights require an immediate shift in diagnostic protocol. Clinicians can no longer assume a negative dengue test represents the end of an epidemiological investigation. Laboratories must integrate Oropouche testing into standard multiplex panels for acute febrile illnesses, especially when evaluating pregnant patients or individuals presenting with unexplained neurological symptoms in endemic regions.
For the general public, the takeaway is not panic, but proactive health management.
-
Seek Timely Medical Care: If you live in or travel to regions with known midges or mosquito activity, do not wait out a severe fever. Early evaluation is critical, particularly if you experience stiff neck, severe light sensitivity, or are pregnant.
-
Enhance Vector Protection: Standard insect repellents containing DEET or Picaridin, tightly woven bed nets, and minimizing skin exposure during peak midge biting hours remain the primary shield against transmission.
Study Limitations and Uncertainties
As with any epidemiological modeling, these findings carry important caveats. The 9.4 million infection estimate relies on mathematical simulations that make standardized assumptions about human immunity, vector behavior, and historical data reporting quality over a 60-year span. Changes in these variables could skew the calculations.
Additionally, while blood-bank antibody data provides an excellent population-wide snapshot of exposure, it cannot pinpoint exactly when an individual was infected or correlate that exposure to specific clinical symptoms. Finally, the estimated 1-in-1,000 severe complication rate is drawn from diagnosed cases; the true complication rate across all infections—including asymptomatic or mild cases that never sought care—remains an open scientific question.
Nevertheless, the core message of the research is undeniable: Oropouche is no longer a minor tropical curiosity. It is a major, established public health challenge hiding in plain sight.
References
-
SciTechDaily. “Hidden Virus May Have Infected 9.4 Million People – Scientists Say We’ve Missed Most Cases.” Published June 26, 2026.
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.







{kind=link}