
ISLAMABAD — A rising number of mpox cases in Pakistan has underscored the severe strain on the country’s already overburdened public health infrastructure. The expanding outbreak has raised urgent concerns among international health authorities and local providers regarding Pakistan’s capacity to manage emerging infectious diseases effectively. The current spike, which features growing clusters of cases in Sindh province alongside isolated infections nationwide, has reignited critical debates over disease surveillance, laboratory diagnostic capacities, and equitable access to care in a landscape where primary healthcare services remain chronically underfunded and unevenly distributed.
What Mpox Is and How It Spreads
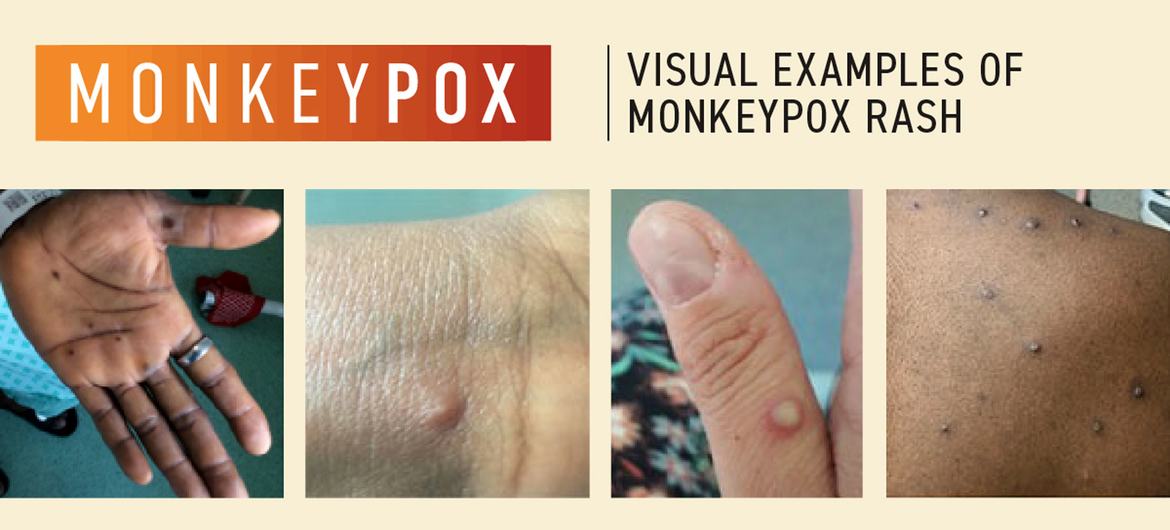
Mpox (formerly known as monkeypox) is a viral zoonotic disease caused by the mpox virus, a member of the Orthopoxvirus genus. According to clinical data from the Aga Khan University Hospital (AKUH), the disease typically manifests with flu-like symptoms—including fever, headache, muscle aches, and swollen lymph nodes—followed by a distinctive rash that evolves from flat spots into fluid-filled blisters, which eventually crust over and scab.
The virus spreads primarily through close, prolonged skin-to-skin contact. This includes direct contact with infectious lesions, body fluids, or contaminated materials such as bedding and clothing. While respiratory droplets can play a role in poorly ventilated or face-to-face settings, epidemiological data confirms it is far less contagious than respiratory viruses like COVID-19 or influenza.
The Current Situation in Pakistan
Pakistan has tracked a small but steadily rising number of confirmed mpox infections since 2023, with the National Institute of Health (NIH) and provincial health authorities monitoring both imported cases and suspected local transmission.
Mpox Regional Distribution in Sindh Province (Early 2026 Data)
┌───────────────────────────────────────┬───────────────────┐
│ District / Focus Area │ Confirmed Cases │
├───────────────────────────────────────┼───────────────────┤
│ Khairpur District (Worst-affected) │ 23 cases │
│ Karachi │ 2 cases │
├───────────────────────────────────────┼───────────────────┤
│ Total Sindh Province Cumulative Tally │ 25 cases │
└───────────────────────────────────────┴───────────────────┘
Health authorities recently flagged at least one case as a confirmed instance of local transmission. This shift indicates that the virus is no longer merely entering the country via returning travelers, but is actively circulating within limited local chains. Tragically, mpox-related deaths have occurred among infants and young children in these clusters. Public health reports indicate these fatalities frequently occurred alongside underlying malnutrition and weakened immunity, rather than from the virus alone.
Public Health Infrastructure Under Pressure
Health experts emphasize that the current mpox cluster represents a broader test of Pakistan’s public health architecture. The national healthcare system, still recovering from the systemic shocks of the COVID-19 pandemic, faces chronic shortages of trained epidemiological staff, diagnostic laboratories, and specialized isolation facilities—particularly across rural and peri-urban areas.
In Sindh, for instance, the Aga Khan University Hospital laboratory had to be urgently pressed into service to provide priority diagnostic testing following the Khairpur cluster. This reliance highlights the scarcity of high-capacity, decentralized diagnostic centers equipped to handle emerging pathogens.
“The recent mpox events show how quickly a localized outbreak can overwhelm existing resources when surveillance, isolation, and contact-tracing systems are not fully integrated or adequately staffed,” notes Dr. Ali Faisal Saleem, Associate Professor and Vice Chair in the Department of Paediatrics and Child Health at Aga Khan University Hospital, Karachi. “Mpox is far less contagious than COVID-19, but it still demands a coordinated response: early detection, rapid isolation of suspected cases, and systematic contact tracing. Any indication of local transmission should trigger an immediate, well-coordinated response.”
Implications for Public Health and Vulnerable Groups
For a low- to middle-income country where large populations depend on overstretched public-sector clinics, mpox introduces a dangerous layer of risk to highly vulnerable demographics. Small children, pregnant women, and individuals living with HIV or other immune-compromising conditions face a significantly higher risk of severe clinical outcomes.
A peer-reviewed analysis published in the Journal of Clinical Virology highlighted that fragile health systems are uniquely vulnerable to the “hidden” costs of outbreaks:
-
Diverted Resources: Shifting personnel away from chronic disease management.
-
Panic-Driven Demand: Overwhelming emergency rooms with low-risk patients.
-
Erosion of Public Trust: Occurring when institutional responses appear delayed or inconsistent.
In Pakistan, these risks are compounded by fragmented data-sharing between federal and provincial health boards, variable regional laboratory capacities, and uneven risk communication. Weak surveillance can delay the early detection of clusters, allowing chains of transmission to go unnoticed until severe cases spill into secondary-care hospitals already operating beyond capacity. This dynamic was explicitly observed in the Khairpur infant cluster, where delayed isolation and background malnutrition contributed to poor clinical outcomes.
What Experts Are Recommending
To mitigate the current surge and insulate the healthcare network against future infectious threats, domestic and international health specialists recommend a multi-pronged strategy:
-
Strengthen Surveillance and Diagnostics: Expand rapid-testing networks to district-level laboratories and integrate mpox into routine infectious-disease reporting systems. Increasing genomic sequencing is vital to distinguish between clades, particularly the more transmissible Clade I variant driving outbreaks globally.
-
Improve Isolation and Infection Control: Ensure major district headquarters hospitals possess functional isolation wards or designated side-rooms, alongside reliable supplies of personal protective equipment (PPE) for frontline medical staff.
-
Scale Up Risk Communication: Deliver clear, consistent public health messaging in local languages regarding symptoms and transmission routes to actively counter misinformation and reduce social stigma.
-
Protect High-Risk Demographics: Reinforce localized nutrition and pediatric immunization programs, strengthen antenatal care, and secure uninterrupted access to antiretroviral therapies for immunocompromised populations.
Limitations and Counterarguments
Some public health critics argue that focusing intensively on mpox in Pakistan may be disproportionate given the country’s overwhelming burden of endemic diseases, such as tuberculosis, severe diarrheal illnesses, and vaccine-preventable childhood infections. They caution that diverting scarce fiscal and human resources toward a relatively small number of mpox cases could inadvertently weaken ongoing campaigns against far more common causes of maternal and infant mortality.
Conversely, proponents of a fortified mpox response counter that building core public health capacities—such as diagnostic frameworks and localized outbreak response units—benefits the entire ecosystem. Strengthening these fundamentals effectively bolsters resilience against both mpox and other emerging or endemic biosecurity threats.
Furthermore, there is an ongoing debate regarding vaccination. While newer mpox-specific vaccines (such as Jynneos) are highly effective, global supplies remain constrained and are primarily directed toward high-income nations. Consequently, vaccine-based prevention is not currently a primary strategy in Pakistan. The national focus must remain on affordable, logistically viable alternatives: aggressive case detection, isolation, and robust contact tracing.
Practical Implications for the Public
For the general public, the primary takeaway from health authorities is vigilance, not panic. Mpox is fundamentally less contagious than airborne respiratory viruses like influenza. Most individuals who contract the virus recover fully at home with standard supportive care, provided they do not have severe underlying medical conditions.
Preventive Guidelines for Families:
-
Seek Immediate Evaluation: Anyone developing a new, unexplained rash, blistering lesions, swollen lymph nodes, or a sudden fever after close contact with a suspected patient should isolate and seek professional medical care.
-
Practice Core Hygiene: Avoid sharing towels, clothing, or bedding with an individual exhibiting a suspicious rash. Maintain frequent hand hygiene using soap and water or alcohol-based sanitizers.
-
Prioritize Routine Health: Ensure children are fully up-to-date on their routine immunizations and receive proper nutritional support to keep their immune systems resilient against opportunistic infections.
Community leaders and local health workers are encouraged to share accurate, evidence-based information to reduce social stigma, ensuring that affected individuals feel safe seeking early diagnostic testing and treatment.
References
- https://tennews.in/rise-in-mpox-cases-in-pakistan-signals-strain-on-public-health-care-infrastructure/#:~:text=Male%2C%20May%2023%20(IANS),effectively%2C%20a%20report%20has%20said.
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.









{kind=link}