

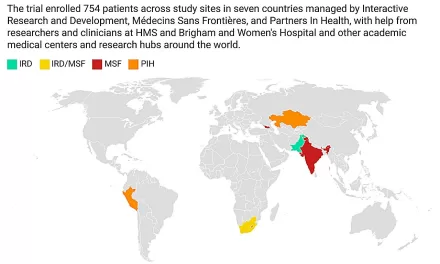
KINSHASA, Democratic Republic of the Congo — A rapidly expanding outbreak of Ebola virus disease in the eastern Democratic Republic of the Congo (DRC) has triggered international mobilization. More than 900 suspected cases, including 101 laboratory-confirmed infections, have been recorded so far, World Health Organization (WHO) Director-General Dr. Tedros Adhanom Ghebreyesus announced. The outbreak, fueled by the rare Bundibugyo strain, is unfolding across the densely populated Ituri Province—home to nearly 5 million people—and has recently crossed the border into neighboring Uganda. Recognizing the acute regional threat, the WHO officially declared the situation a Public Health Emergency of International Concern (PHEIC) on May 16, 2026.
The Velocity of the Outbreak
According to the WHO’s latest epidemiological situation reports, the number of laboratory-confirmed cases remains in the double digits, but suspected cases have surged dramatically. In mid-May, health authorities tracked fewer than 250 suspected infections; by late May, that number surpassed 900.
Most of these suspected cases are heavily clustered within Ituri Province. Epidemiologists report that a combination of dense local populations, poor road infrastructure, and intense regional mobility is accelerating viral transmission. Adding to the gravity of the situation, Ugandan health authorities have confirmed a small number of imported cases linked to travelers arriving from the DRC, transforming a localized crisis into an urgent regional threat.
Outbreak At-a-Glance (May 2026)
+-----------------------------------+-----------------------------------+
| Metric | Status / Value |
+-----------------------------------+-----------------------------------+
| Total Suspected Cases | 900+ |
| Laboratory-Confirmed Cases | 101 |
| Primary Epicenter | Ituri Province, DRC |
| Cross-Border Transmission | Confirmed (Uganda) |
| Estimated Case-Fatality Rate | ~33% |
+-----------------------------------+-----------------------------------+
Understanding the Bundibugyo Strain
Ebola virus disease is caused by several distinct species within the Filoviridae family. The Bundibugyo ebolavirus was first identified in 2007 during an outbreak in the Bundibugyo District of western Uganda. While it is historically less frequently reported than the highly lethal Zaire strain, it remains a severe public health threat.
The virus causes acute hemorrhagic fever. Early symptoms are often indistinguishable from other tropical diseases like malaria or typhoid, presenting as:
-
High fever and profound muscle pain
-
Severe headache and sore throat
-
Vomiting and debilitating diarrhea
-
In advanced stages: internal and external bleeding, followed by multi-organ failure.
The most critical challenge of this outbreak lies in the medical countermeasure landscape. While the global health community successfully developed and deployed highly effective vaccines (such as Ervebo) and monoclonal antibody treatments (like Inmazeb and Ebanga) to combat the Zaire strain during recent outbreaks, these therapies do not offer cross-protection against the Bundibugyo variant. Consequently, there is currently no licensed vaccine or specific antiviral therapy available for this strain. Although international research consortia are fast-tracking candidate vaccines and therapeutic molecules into clinical evaluation, none have completed regulatory approval as of mid-2026.
WHO Risk Assessment and Global Response
The declaration of a Public Health Emergency of International Concern (PHEIC) represents the WHO’s highest level of global alert. It signifies that an extraordinary health event poses a transboundary risk and demands a highly coordinated international financial and technical response.
Following the declaration, the WHO elevated its internal risk assessment for the DRC to “very high,” while rating the regional risk for neighboring East African nations as “high.” The global risk level currently remains “low.”
The agency emphasized that the intersection of a highly vulnerable, displaced population and an active, long-standing armed conflict in eastern DRC creates a volatile environment. These factors significantly elevate the likelihood of uncontrolled viral replication and further cross-border spillover.
Operational Realities on the Ground
Implementing infection prevention and control measures in Ituri Province presents severe operational challenges for frontline humanitarian teams. Decades of geopolitical instability have left local healthcare infrastructure severely weakened. Furthermore, conflict-driven population displacements mean that thousands of individuals live in temporary, overcrowded settlements where hygiene measures are difficult to maintain.
Key Field Challenges:
1. Pervasive community distrust stemming from historical conflicts.
2. Intermittent violence restricting humanitarian access to remote villages.
3. Severe deficits in localized laboratory and diagnostic infrastructure.
Public health workers report that deep-seated community distrust—intensified by years of military conflict and fatigue from previous health interventions—is hindering contact tracing efforts. Families are sometimes reluctant to report symptomatic loved ones or adhere to mandated safe and dignified burial protocols. To curb transmission, local authorities have temporarily restricted high-density community gatherings, including regional football matches and traditional funeral ceremonies, which have historically served as super-spreader events.
Expert Perspectives
Medical experts emphasize that the official numbers likely represent only a fraction of the actual burden of disease. Dr. Anne Ancia, the WHO Representative in the DRC, briefed reporters in Geneva on the visibility gap:
“Our frontline teams are seeing hundreds of suspected cases and dozens of suspected deaths in communities, yet our laboratory confirmation capacity remains constrained by logistics and security. We know the epidemic is much larger than the confirmed numbers suggest.”
Independent public health authorities note that the lack of a biological shield changes the nature of the containment strategy. Dr. Peter Salama, a specialist in international epidemic response who is not involved in the current deployment, noted that standard containment mechanics must now do all the heavy lifting:
“The absence of a licensed Bundibugyo vaccine removes one of the most powerful pharmaceutical tools we relied upon in recent Zaire-strain outbreaks. Without ring vaccination to halt transmission chains, the backbone of this response must rely entirely on classic public health fundamentals: rapid isolation, rigorous contact tracing, community engagement, and early supportive care.”
Public Health Implications and Uncertainties
The rapid trajectory of suspected infections serves as an urgent reminder of how quickly an unmitigated filovirus can spread within conflict zones. Because the margin for error is narrow, a single undetected transmission chain or a lapse in border surveillance can easily compromise containment progress. For neighboring nations—including Uganda, Rwanda, and South Sudan—the immediate priorities involve fortifying cross-border screening checkpoints, establishing isolation wards, and distributing rapid diagnostic test kits.
However, significant epidemiological uncertainties remain. Because more than 80% of the reported figures are classified as “suspected,” the exact geographic boundaries of the outbreak are difficult to pin down. Intensive laboratory testing will inevitably rule out some patients who are suffering from malaria or cholera. Conversely, due to the remote nature of many villages in Ituri, other true Ebola cases may go entirely unrecorded.
Crucially, clinical data shows that the case-fatality rate for the Bundibugyo strain hovers around 33%. Medical literature highlights that early supportive clinical care—consisting of aggressive intravenous rehydration, electrolyte stabilization, and targeted symptom management—can substantially improve individual survival outcomes. The overriding challenge in eastern DRC is ensuring that patients can safely reach these specialized treatment units in time.
Guidance for the Public and International Travelers
For individuals residing in or traveling through the affected provinces of the DRC and neighboring border regions, health agencies advise strict adherence to infection prevention protocols:
-
Avoid Direct Contact: Stay away from the blood, body fluids (such as saliva, sweat, or vomit), or personal items of anyone showing symptoms of unexplained illness.
-
Practice Strict Hygiene: Frequently wash hands with soap and clean water or utilize alcohol-based hand rubs.
-
Monitor Health Status: Residents should monitor for sudden onset of fever, extreme fatigue, or unusual bruising, and report symptoms immediately to local health facilities.
-
Traveler Awareness: Anyone who has recently traveled to Ituri Province or adjacent areas and develops compatible symptoms should self-isolate immediately, seek professional medical evaluation, and explicitly disclose their complete travel history to clinicians.
For the international public, global health authorities emphasize that the risk of intercontinental spread remains low. Standard border screening measures and rapid isolation protocols at international transit hubs are highly effective at mitigating long-distance transmission. The WHO continues to explicitly advise against international travel or trade restrictions, advocating instead for targeted border health surveillance and well-funded regional containment operations.
Medical Disclaimer
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.
References
-
Reuters. (May 24, 2026). More than 900 suspected Ebola cases identified in DRC, WHO chief says.










{kind=link}