
NEW DELHI — In what public health experts are calling a monumental shift in global healthcare delivery, India’s Ayushman Bharat Digital Mission (ABDM) has established one of the world’s largest integrated digital health networks. Fresh government data reveals that the initiative has cross-referenced more than 104 crore (1.04 billion) digital health records with over 93 crore (930 million) individually verified Ayushman Bharat Health Accounts (ABHA).
By establishing a single interoperable highway, the initiative connects patients, hospitals, pharmacies, and insurance providers on a unified network. The system aims to eliminate physical paperwork, slash hospital registration queues, and lay the groundwork for an advanced public health data infrastructure.
Redefining the Patient Experience: From Hours to Minutes
For decades, navigating the checkout, billing, and registration processes in overcrowded public and private hospitals across India meant enduring hours of administrative gridlock. Emerging data suggests that smartphone-enabled systems are aggressively dismantling these wait times.
According to a comprehensive evaluation conducted by the Indian Institute of Health Management Research (IIHMR), the National Health Authority’s (NHA) “Scan and Share” service—a system allowing patients to scan a unique QR code at hospital entrances to instantly populate administrative intake forms—has fundamentally changed outpatient department (OPD) workflows.
Key Finding (IIHMR Study): The implementation of automated QR token registration reduced the average patient waiting time in hospital lobbies from approximately 60 minutes down to between 2 and 5 minutes.
As of June 2026, healthcare facilities nationwide have issued more than 23.21 crore ABHA-linked digital tokens. By pulling standardized demographic data directly from a citizen’s secure ABHA profile, hospitals bypass manual data entry entirely, avoiding clerical errors while optimizing resource allocation.
The Architecture of India’s Digital Backbone
The mission relies on a modular framework of public digital goods designed to link highly fragmented elements of the healthcare landscape into an interconnected network:
┌────────────────────────────────────────┐
│ ABHA Number │
│ (14-Digit Unique Health Identity) │
└───────────────────┬────────────────────┘
│
┌─────────────────────────┼─────────────────────────┐
▼ ▼ ▼
┌───────────────────────┐ ┌───────────────────────┐ ┌───────────────────────┐
│ Healthcare Providers │ │ Health Facilities │ │ Unified Health Inter. │
│ (HPR Registry) │ │ (HFR Registry) │ │ (UHI Open Apps) │
└───────────────────────┘ └───────────────────────┘ └───────────────────────┘
-
Ayushman Bharat Health Account (ABHA): A 14-digit unique health identifier that serves as the citizen’s medical identity, mapping diagnostic data, prescriptions, and historical discharge summaries across multiple providers.
-
Healthcare Professionals Registry (HPR) & Health Facility Registry (HFR): Verified, centralized repositories ensuring that only certified doctors, AYUSH practitioners, clinics, and laboratories can participate in the data exchange network.
-
Unified Health Interface (UHI): Mirroring the frictionless protocol of India’s Unified Payments Interface (UPI) for financial transactions, UHI acts as an open network. It allows consumers to discover providers, schedule teleconsultations, check real-time blood bank stocks via e-RaktKosh, and book ambulances seamlessly across different consumer applications.
Upgrading Consumer Access: The Aarogya Setu Overhaul
To bridge the gap between high-tech infrastructure and citizen utility, the Ministry of Health and Family Welfare introduced Aarogya Setu 2.0. Originally deployed as a contact-tracing application during the COVID-19 pandemic, the revamped application serves as a comprehensive personal health record platform.
The application integrates advanced toolsets, including Optical Character Recognition (OCR) systems that parse physical diagnostic paperwork into “Smart Reports” and machine-readable biological markers. It also aggregates consumer health data by syncing directly with personal wearable devices to log continuous vitals like heart rate, daily caloric expenditure, and ambient glucose fluctuations.
Crucially, the upgrade interfaces with the National Health Claims Exchange (NHCX). This gives users a direct visual pipeline into their Ayushman Bharat-Pradhan Mantri Jan Arogya Yojana (AB-PMJAY) government health wallets alongside private insurance policies, providing upfront transparency regarding coverage terms and active claim statuses.
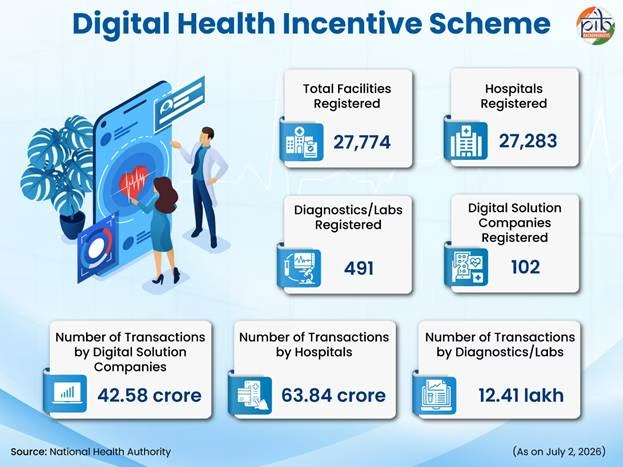
Incentivizing the Private Sector and Small Clinics
A historic hurdle for national digital health programs globally has been the slow adoption rate among private practitioners and small, rural clinics. To counteract this, the Indian government introduced the Digital Health Incentive Scheme (DHIS), offering direct financial reimbursements to facilities that create and link digitized health records.
According to financial disclosures, the government has distributed substantial capital incentives to catalyze adoption:
| Facility Classification | Cumulative Incentive Disbursements (INR) |
| Hospitals & Medical Centers | Rs. 107+ Crore |
| Digital Solution Companies (DSCs) | Rs. 26+ Crore |
| Diagnostics, Laboratories, & Pharmacies | Rs. 2.95 Crore |
To simplify compliance for standalone practitioners, the government launched eSushrut@Clinic, a lightweight, plug-and-play Hospital Management Information System (HMIS). Developed by the Centre for Development of Advanced Computing (C-DAC), this standardized, low-cost platform automates billing, scheduling, and digital charting. Over 2,200 small-scale facilities have already integrated into the cloud ecosystem through this module.
Data Privacy, Security, and the Medical AI Push
The collection of vast quantities of medical records naturally raises pressing ethical questions regarding patient surveillance and corporate data exploitation.
Public health officials emphasize that ABDM utilizes a strict “Privacy-by-Design” architecture. There is no centralized government super-server storing raw medical records. Instead, patient data remains distributed at the edge, residing exclusively with the specific hospital, laboratory, or doctor that generated the file.
Data transfer occurs on a revocable, time-bound consent model. A specialist in another city cannot view a patient’s historical records unless the patient explicitly approves a digital permission request via their smartphone. Furthermore, any consumer application or third-party platform attempting to integrate with the ABDM network must pass a simulated environment evaluation within a dedicated technical “sandbox” and clear exhaustive independent cybersecurity audits.
Anonymized aggregates derived from this vast digital ecosystem are also driving advancements in medical Artificial Intelligence (AI). Under the recently launched Strategy for Artificial Intelligence in Healthcare for India (SAHI) and the Benchmarking Open Data Platform for Health AI (BODH), developers can train machine learning diagnostic models on-site using a secure, federated ecosystem. This methodology ensures raw patient identities remain protected while refining algorithmic model weights to predict public health anomalies and optimize localized disease surveillance.
Infrastructure Challenges and Public Health Realities
While the scale of the digital rollout is mathematically unprecedented, independent health commentators urge cautious optimism.
Medical analysts note that deep infrastructure deficits persist between tier-one urban metropolises and marginalized rural landscapes. While an urban diagnostic chain can seamlessly process records via the NHCX, thousands of primary health sub-centers in remote geographies still struggle with basic cellular connectivity and regular power cuts.
Additionally, achieving true digital parity requires sustained training for healthcare staff and comprehensive outreach to populations with limited digital literacy. Critics emphasize that digital public infrastructure must remain an accelerator for care delivery, rather than an administrative barrier that inadvertently excludes citizens who lack access to modern technology.
As the National Health Authority aims to onboard remaining offline clinics, the coming years will determine how successfully India converts this unprecedented digital framework into measurable improvements in clinical outcomes for its entire population.
References
https://www.pib.gov.in/PressReleasePage.aspx?PRID=2281466®=48&lang=1
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.










{kind=link}