
LONDON — In a historic shift aimed at transforming how the world’s most common hormonal disorder is understood, treated, and researched, an international consortium of medical authorities has officially proposed a new name for polycystic ovary syndrome (PCOS). The condition will now be known as polyendocrine metabolic ovarian syndrome, or PMOS.
The landmark proposal, published in The Lancet, follows a massive, multi-step global consensus process designed to correct a decades-old medical misnomer. For generations, the name “polycystic ovary syndrome” has led patients and primary care physicians to focus narrowly on the ovaries. However, the condition is actually a complex, multisystem disorder. Leading health organizations estimate that the condition affects approximately one in eight women and individuals assigned female at birth worldwide—amounting to more than 170 million people.
While proponents hail the change as a vital leap forward for scientific accuracy and patient dignity, the announcement has sparked an intense debate within the medical community. Critics question whether altering a name will truly solve the systemic barriers to care, or simply introduce new bureaucratic hurdles for a vulnerable patient population.
Correcting a Decades-Old Misnomer
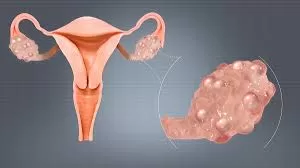
The push to replace PCOS with PMOS stems from a fundamental mismatch between the condition’s name and its underlying biology. The term “polycystic ovary syndrome” was popularized in the mid-20th century because many patients presented with multiple fluid-filled sacs in their ovaries.
However, modern endocrinology has proven that these are not abnormal cysts in the traditional sense; rather, they are partially developed follicles that have stalled due to hormonal imbalances. Furthermore, a person can have the condition without ever developing these follicles, and conversely, healthy individuals can have them without having the disorder.
The consensus paper in The Lancet outlines a rigorous, years-long consultation process led by the Global Name Change Consortium. The group gathered 14,360 survey responses from patients and clinicians across the globe and secured the endorsement of 56 major academic, clinical, and patient advocacy organizations.
According to the consortium, the new name—polyendocrine metabolic ovarian syndrome—was selected based on four core criteria: scientific accuracy, clarity, cultural appropriateness, and feasibility. By intentionally removing the word “cysts” and introducing “endocrine” and “metabolic,” the new terminology shifts the focus toward the complex hormonal framework that drives the disease.
Why Doctors and Advocates Are Split
Reaction to the rollout of PMOS highlights a deep division among health experts regarding the practical utility of medical rebranding.
The Case for PMOS: Visibility and Accuracy
Supporters argue that language acts as the first gatekeeper to effective healthcare. “For too long, this condition has been reduced to a misunderstanding about cysts and ovaries,” noted representatives from the Endocrine Society in a supportive statement. Proponents emphasize that a more accurate name will encourage primary care doctors to look beyond reproductive health, leading to earlier interventions for metabolic complications.
“The old name led to profound misunderstanding among both patients and clinicians,” said Dr. Helena Teede, an endocrinologist who led the global consensus process. “A name change is fundamentally needed to reflect the true complexity of the condition, reduce the stigma of infertility associated with the word ‘ovary,’ and ensure patients receive comprehensive care.”
The Case for Caution: Implementation and Confusion
However, not all experts are convinced that a new acronym is the answer. Skeptics argue that a consensus statement alone cannot alter the daily realities of clinical practice. Critics point out that updating diagnostic codes, electronic health records, insurance reimbursement frameworks, and medical school curricula takes years and millions of dollars.
There is also concern that changing the name before establishing standardized, cross-disciplinary clinical pathways puts the cart before the horse. During the lengthy transition period, patients may become confused, potentially leading to fragmented care if their primary doctor uses the new terminology while their gynecologist sticks to the old framework.
The Public Health Stakes
From a public health perspective, the stakes could not be higher. PMOS is a leading cause of infertility, but its reach extends far beyond reproduction. The condition is intrinsically linked to insulin resistance, a metabolic malfunction where the body’s cells do not respond properly to insulin. This puts individuals with PMOS at a significantly elevated risk for:
-
Type 2 diabetes
-
Cardiovascular disease and hypertension
-
Nonalcoholic fatty liver disease
-
Endometrial cancer
-
Mental health challenges, including severe anxiety and depression
Because the symptoms are so diverse—ranging from irregular periods and fertility struggles to acne, excess facial hair growth (hirsutism), and unexplained weight gain—patients frequently spend years bouncing between dermatologists, gynecologists, and weight-loss clinics before receiving a correct diagnosis.
[Patient Symptoms] ──> Fragmented Specialists (Dermatology / Gynecology)
│
▼
[Delayed Diagnosis]
│
(New PMOS Framework Aims to Fix This)
│
▼
[Integrated Care] ──> Comprehensive Screening (Metabolic / Endocrine / Mental Health)
A name that explicitly highlights “endocrine” and “metabolic” factors signals to frontline clinicians that these patients require routine screenings for cardiovascular and blood sugar issues, rather than just treatments to regulate their menstrual cycles.
What PMOS Means for Patients Today
For individuals currently diagnosed with PCOS, experts emphasize that this announcement should not cause alarm.
The underlying health issue has not changed; only the medical label is evolving.
Patients do not need to rush to alter their existing treatment plans. Current management strategies—which often include lifestyle modifications, metformin for insulin sensitivity, hormonal contraceptives for cycle regulation, and targeted fertility treatments—remain entirely valid.
Instead, patients should use this global conversation as an opportunity to evaluate their current care. The critical question to discuss with a healthcare provider is whether all facets of the condition are being addressed. If a treatment plan focuses solely on fertility or acne, it may be time to ask about metabolic health screenings, long-term cardiovascular risks, and psychological well-being.
The medical community is preparing for a gradual, multi-year transition. Patients should expect to see both PCOS and PMOS used interchangeably on educational materials, advocacy websites, and medical charts as the global healthcare infrastructure slowly adjusts to the new terminology.
The Hard Road to Implementation
The true test of the PMOS nomenclature will lie in its real-world implementation. While the Global Name Change Consortium achieved an unprecedented level of international cooperation, a consensus paper cannot mandate institutional adoption.
Over the coming years, major bodies such as the World Health Organization (WHO) will need to integrate PMOS into official diagnostic coding systems like the International Classification of Diseases (ICD). Furthermore, clinical trial registries and research funding agencies must adopt the terms to prevent the scientific literature from becoming fragmented.
Ultimately, the shift to PMOS underscores a growing recognition that medical language is far from cosmetic. When a disease affecting 170 million people is poorly named, it directly impacts whether patients are believed, how resources are allocated for research, and how comprehensively care is delivered. Whether PMOS achieves its ambitious goals depends entirely on how effectively the global health system translates this semantic shift into clinical practice.
References
- https://www.medscape.com/viewarticle/critics-question-science-and-process-behind-new-term-pcos-2026a1000lr2
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.







{kind=link}