
BENGALURU — In a major step forward for digital health, a researcher based in Bengaluru has developed artificial intelligence (AI) models capable of identifying women at a higher risk of developing cervical cancer. The predictive algorithms analyze a combination of patient clinical data and medical imagery to flag vulnerabilities years before physical tumors form. While the breakthrough adds to a compelling body of global evidence supporting automated screening, public health experts emphasize that the technology must still prove its dependability in real-world clinical settings before widespread deployment.
The research, led by Lalasa Mukku, a doctoral researcher at Christ (Deemed-to-be-University) in Bengaluru, introduces a non-invasive digital layer to traditional gynecological screenings. Notably, Mukku holds patents for an AI model designed to predict cervical cancer risk up to five years prior to tumor development. Although still in the investigational phase, the technology arrives at a crucial moment as global health organizations scramble to solve persistent shortages of trained medical specialists in low- and middle-income regions.
Inside the Technology: What the Data Shows
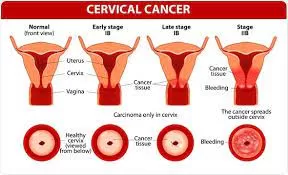
The core of this new diagnostic approach focuses on detecting Cervical Intraepithelial Neoplasia (CIN). CIN refers to precancerous, abnormal changes occurring in the squamous cells on the surface of the cervix. If left unmonitored or untreated, these lesions can progress into invasive cervical cancer over a span of several years. Because these cellular transformations happen slowly and silently, early detection offers a nearly 90% five-year survival rate, according to historical oncological data. However, standard visual assessments are frequently prone to human error or limited by subjective interpretation.
Mukku’s method bridges this gap by combining patient medical history with multimodal time-series images captured during a standard colposcopy examination. During a colposcopy, clinicians inspect the cervix after sequentially applying saline, acetic acid, and Lugol’s iodine solutions. Each agent alters how the tissue reflects light, causing abnormal areas to stand out.
One of the prominent technical hurdles in automated colposcopy is “specular reflection”—bright reflections caused by moisture on the cervix that algorithms can easily mistake for white precancerous lesions. To solve this, Mukku developed a dedicated preprocessing technique to digitally isolate the cervix and strip away these visual artifacts before analysis.
The analytical performance of these systems across different research phases demonstrates strong statistical promise:
| Research Study / Publication | AI Architecture Utilized | Key Methodological Feature | Reported Diagnostic Accuracy |
| Int. Journal of Advances in Intelligent Informatics (2024) | CMT-CNN (Colposcopic Multimodal Temporal Convolutional Neural Network) | Integrates sequential colposcopy images (saline, acid, iodine) with patient history. | 92.3% |
| IEEE Conference Presentation (2025) | Quantum Convolutional Neural Network (QCNN) | Evaluated on highly standardized, publicly available screening datasets. | 98.6% |
The Public Health Imperative: Bridging the Screening Gap
Cervical cancer remains one of the most prominent public health challenges worldwide, claiming hundreds of thousands of lives annually. The burden is heavily skewed toward resource-constrained settings where access to experienced pathologists, regular Pap smears, and dedicated colposcopists is highly scarce.
According to a comprehensive 2024 review published in Cancer Biology & Medicine, the World Health Organization (WHO) has established an ambitious “90-70-90” target for 2030, which mandates screening 70% of women globally using a high-performance test between the ages of 35 and 45. Currently, many developing countries remain far below this threshold.
In countries like India—which historically recorded over 123,000 new cases and approximately 77,000 deaths annually according to past GLOBOCAN registry data—preventative framework implementation requires massive scalability. The automation, objectivity, and rapid processing speed offered by deep learning frameworks could allow local clinics to triaging high-risk individuals effectively, maximizing the impact of limited specialist resources.
The Road from the Lab to the Clinic: Expert Caution
Despite the impressive 92.3% and 98.6% accuracy rates reported in research papers, medical experts not involved in the studies urge the public and healthcare communities to temper their expectations with clinical realism. A fundamental truth of medical AI is that laboratory performance rarely translates seamlessly to the chaotic environment of a busy hospital.
The 2024 Cancer Biology & Medicine global review, co-authored by researchers affiliated with the WHO’s International Agency for Research on Cancer (IARC), confirms that while AI significantly strengthens early detection pipelines, “further exploration and validation are needed” before population-level implementation can occur.
The primary limitation rests on data bias and environmental variability. AI models trained on perfectly curated public datasets often falter when introduced to different hospital settings. Subtle differences in clinic lighting, variations in colposcope camera hardware, diverse patient demographics, and inconsistencies in chemical application protocols can degrade algorithmic accuracy. To prove their true clinical utility, these models must undergo rigorous, large-scale prospective clinical trials across multiple institutions.
The Evolving Prevention Toolkit: What Patients Need to Know
For the average patient, this technological evolution is not a signal to abandon traditional healthcare pathways, but rather a preview of an added layer of clinical support. AI is designed to augment doctors, helping them reduce missed lesions and prioritize suspicious cases more accurately, rather than replacing human clinical judgment.
Crucially, global health authorities remind the public that cervical cancer is highly preventable through an established, four-pillar toolkit:
-
Human Papillomavirus (HPV) Vaccination: Protecting individuals against the viral strains responsible for the vast majority of cervical cellular abnormalities.
-
Routine Screening: Regular Pap tests or high-performance HPV DNA testing.
-
Early Diagnosis: Timely colposcopies and targeted biopsies when screening anomalies appear.
-
Prompt Treatment: Treating low- or high-grade precancerous lesions before they advance.
As India continues its nationwide expansion of the HPV vaccination rollout, combining robust primary prevention with emerging digital diagnostic aids could dramatically alter the disease’s trajectory. The most vital takeaway for women remains clear: because precancerous cervical changes are fundamentally silent and produce no early warning signs, routine screening must not be delayed until symptoms surface.
References
- https://health.economictimes.indiatimes.com/news/diagnostics/bengaluru-research-uses-ai-to-hunt-cervical-cancer-risk-years-before-diagnosis/132060934?utm_source=latest_news&utm_medium=homepage
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.








{kind=link}