

KAMPALA, Uganda — In a major step toward regional health security, the Africa Centres for Disease Control and Prevention (Africa CDC), the World Health Organization (WHO) Regional Office for Africa, and the Ugandan government officially launched a co-located Joint Continental Incident Management Support Team (IMST) on June 29, 2026. Headquartered at the Infectious Diseases Institute at Makerere University in Kampala, this unified operational platform is tasked with coordinating containment and preparedness efforts for the ongoing Bundibugyo Ebola virus outbreak currently affecting the Democratic Republic of Congo (DRC) and Uganda. By pulling together top-tier technical experts under one roof, the initiative aims to halt cross-border transmission through unified surveillance, synchronized logistics, and aggressive community engagement.
A Unified Hub for Rapid Deployment
The creation of the IMST marks a shift away from fragmented national responses toward an integrated regional strategy. By establishing a single, co-located coordination hub, the initiative brings together technical experts from Africa CDC, WHO AFRO, and various international partner organizations. This team will directly support country-led outbreak responses across several critical areas, including operational planning, disease surveillance, case management, logistics, and risk communication.
The strategic choice of Makerere University as the host institution allows the IMST to provide rapid technical assistance and real-time data analysis not only to the DRC and Uganda but also to neighboring countries deemed at high risk for viral spillover.
This operational hub complements a broader, six-month continental preparedness and response plan spanning June to November 2026. The ambitious initiative aims to raise $518 million to scale up laboratory testing, strengthen infection prevention and control (IPC) measures, optimize clinical care, and stabilize volatile transmission chains.
“One Plan, One Budget, One Team”
Public health leadership has emphasized that a fragmented approach is no longer viable in an interconnected region where infections frequently cross porous borders. WHO leadership framed the joint plan as an essential evolution in outbreak management, advocating for a strict “one plan, one budget, one team” approach. Experts argue that coordinated partnership under the explicit leadership of the affected countries is the only definitive way to control viral spread and safeguard vulnerable populations.
According to statements from Africa CDC and the WHO, co-location will fundamentally alter the logistics of the response. Integrating technical teams into a single physical space is expected to shorten decision cycles, streamline information sharing, and eliminate the costly duplication of efforts that historically slows down cross-border emergency interventions.
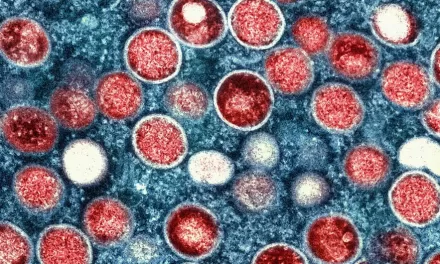
The Bundibugyo Challenge: No Vaccines, No Therapeutics
The urgency surrounding the IMST’s launch is heightened by the specific biology of the pathogen. The current outbreak is driven by the Bundibugyo species of the Ebola virus, which is genetically distinct from the more widely known Zaire species.
Unlike the Zaire virus—which benefited from the development of highly effective vaccines (such as Ervebo) and monoclonal antibody treatments during past outbreaks—the Bundibugyo species has no widely licensed species-specific vaccines or therapeutics. This scientific gap significantly elevates the stakes for traditional public health interventions, putting the weight of containment entirely on rapid detection, meticulous contact tracing, and rigorous infection prevention in healthcare settings.
+-----------------------------------------------------------------------------+
| BUNDIBUGYO EBOLA OUTBREAK |
| Continental Response Framework |
+-----------------------------------------------------------------------------+
| Operational Timeline: June – November 2026 |
| Funding Target: $518 Million USD |
| Core Objective: Support emergency coordination, laboratory scaling, IPC, |
| case management, and community engagement. |
+-----------------------------------------------------------------------------+
Compounding the biological challenge is the complex humanitarian landscape in the region. Recent field reports from eastern DRC have raised alarms regarding rapid community spread and substantial under-detection, particularly within displaced populations. Humanitarian camps face severe challenges, including limited sanitation infrastructure, deep-seated community resistance to medical testing, and a sharp reduction in international water, hygiene, and sanitation (WASH) funding, all of which create ideal conditions for sustained viral transmission.
Public Health Implications and Operational Realities
The primary public health objective of the IMST is to prevent a localized crisis from blowing up into a broader pan-African emergency. By aligning surveillance, laboratory networks, and supply chains under a singular operational roof, health authorities hope to dramatically accelerate case detection and streamline clinical referrals.
However, historical precedents in Ebola management demonstrate that centralized command structures have inherent limitations. Public health analysts point out that while a centralized hub can optimize resource allocation, its ultimate success depends on the willingness of local authorities to share real-time data and the willingness of local communities to trust external interventions.
Where community resistance to testing persists or basic sanitation is non-existent, a central hub cannot stop transmission on its own. The IMST’s heavy reliance on supportive clinical care and strict isolation measures underscores a pragmatic but frustrating reality: without species-specific biomedical tools, traditional community-level public health work remains the primary line of defense.
What This Means for Communities and Clinicians
For frontline healthcare workers and public health professionals operating in East and Central Africa, the activation of the IMST provides a clearer framework for obtaining technical guidance. Clinicians can expect streamlined access to surge resources, standardized protocols for case management, and harmonized IPC guidelines distributed through a singular, authoritative channel.
For the general public, health authorities emphasize that basic, proactive behaviors remain highly effective at preventing infection:
-
Understand Transmission: Ebola viruses spread through direct contact with the bodily fluids (such as blood, saliva, or sweat) of an infected person or through contaminated surfaces.
-
Prompt Care-Seeking: Individuals exhibiting compatible symptoms—such as sudden fever, intense weakness, muscle pain, vomiting, or unexplained bleeding—should seek medical evaluation immediately, as early supportive care dramatically improves survival rates.
-
Respect Public Health Guidance: Adhering to local guidance regarding safe, dignified burials and voluntary testing is essential to breaking transmission chains.
-
Participate Responsibly: Community members should engage with vaccination campaigns or clinical trial efforts only when explicitly offered and recommended by recognized, local health authorities.
References
Institutional Statements & Press Releases
-
WHO AFRO: “WHO, Africa CDC launch Continental Incident Management Support Team to strengthen coordination for Ebola outbreak response,” published June 28, 2026.
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.








{kind=link}