
Situation at a Glance
Description of the Situation
Between 26 and 28 January 2024, the Cambodia IHR NFP notified WHO of two confirmed cases of human infection with avian influenza A (H5N1) virus. These cases were reported from Kampong Trabek district, Prey Veng province, and Puok district, Siem Reap province, Cambodia.
The first case, a 3-year-old, was reported on 26 January 2024, from Kampong Trabek district, Prey Veng province. The patient developed symptoms on 13 January 2024 and was admitted to hospital on 16 January 2024 with high fever, cough and runny nose. Samples were collected at the hospital and were transported to the National Institute of Public Health for testing. There, the samples tested positive for H5N1 through quantitative reverse transcription polymerase chain reaction (RT-qPCR) on 25 January 2024 and were confirmed by the Institut Pasteur du Cambodge (IPC) on 25 January 2024. The patient had a history of exposure to backyard chickens that were found dead around the residence. A total of 14 close contacts of the case were identified and samples were collected and tested, of which none were positive for influenza.
The second case, a 69-year-old, was reported on 28 January 2024, from Puok district, Siem Reap province, Cambodia. The patient had pre-existing hypertension and had onset of symptoms on 21 January 2024, including a fever exceeding 38°C, cough, and difficulty breathing. The patient was admitted to the hospital on 23 January 2024 and tested positive for H5N1 through RT-PCR at the National Institute for Public Health on 27 January 2024. The sample was confirmed positive by additional testing at IPC on 28 January 2024. Based on the initial investigation, the patient raised domestic poultry and fighting roosters. Three chickens tested were found to be positive for influenza A(H5N1). No sampling and testing of the environment was done. Four close contacts and 39 additional contacts were identified and tested, of which one was found positive for an unrelated influenza B/Victoria lineage.
The two confirmed cases of human infection with avian influenza A (H5N1) virus have since recovered. Genome sequencing and phylogenetic analysis revealed that the HA genes of A/H5 isolates in both confirmed cases belong to clade 2.3.2.1c.
In 2023, six human cases, including four deaths, were reported from Kampot Province (n=2), Prey Veng Province (n=3) and Svay Rieng (n=1). From 2003 through 28 January 2024, a total of 64 cases of human infection with influenza A(H5N1), including 41 deaths, have been reported from Cambodia.
Epidemiology
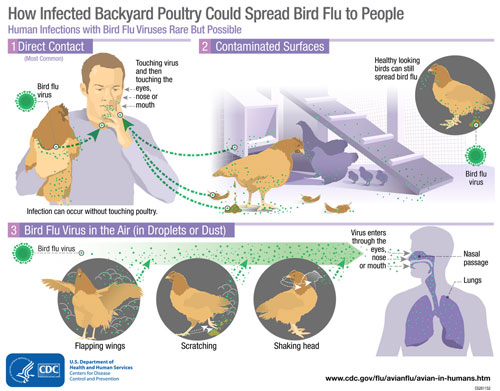
Animal influenza viruses normally circulate in animals but can also infect humans. Infections in humans have primarily been acquired through direct contact with infected animals or contaminated environments. Depending on the original host, animal influenza A viruses can be classified as avian influenza, swine influenza, or other types of animal influenza viruses.
Avian, swine, and other animal influenza virus infections in humans may cause disease ranging from mild upper respiratory tract infection to more severe disease and death. Conjunctivitis, gastrointestinal symptoms, encephalitis and encephalopathy have been reported. There have also been several detections of influenza A(H5N1) virus in asymptomatic persons. These detections were made because the individuals had exposure to infected birds as they were involved in poultry farms depopulation/decontamination procedures following reported poultry outbreaks.
Laboratory tests are required to diagnose human infection with influenza. WHO periodically updates technical guidance protocols for the detection of zoonotic influenza using molecular methods, e.g. reverse transcription polymerase chain reaction (RT-PCR). Evidence suggests that some antiviral drugs, notably neuraminidase inhibitors (oseltamivir, zanamivir), can reduce the duration of viral replication and improve prospects of survival in some cases.
Public Health Response
The Cambodia Ministry of Health’s national and sub-national rapid response teams, with support from the Ministry of Agriculture, Forestry and Fisheries, and the Ministry of Environment, have been actively investigating the avian influenza outbreak in the Prey Veng and Siem Reap Provinces.
Ongoing efforts involve investigations to find sources and modes of transmission in both animals and humans. Additionally, there is a continuing search for suspected cases and contacts to prevent any possibility of onward transmission. Poultry samples have been collected and testing is ongoing.
WHO Risk Assessment
From 2003 to 28 January 2024, 884 human cases of influenza A (H5N1) infection, including 461 deaths, have been reported globally from 23 countries. Almost all cases of human infection with avian influenza A(H5N1) were sporadic infections and have been linked to close contact with infected live or dead birds, or influenza A(H5N1) contaminated environments. These animal influenza viruses do not easily infect humans, and human-to-human transmission appears to be unusual. However, severe disease with high mortality rates can occur as a result of human infection. Given that the virus continues to circulate in poultry, particularly in rural areas in Cambodia and other countries where the virus is endemic in poultry, the potential for further sporadic human cases can be expected.
Available epidemiological and virological evidence suggests that A(H5N1) viruses have not acquired the ability to sustain transmission among humans. Therefore, the likelihood of human-to-human spread is considered low. Based on available information, WHO assesses the risk to the general population posed by this virus to be low. The risk assessment will be reviewed as needed if additional information becomes available.
Close analysis of the epidemiological situation, further characterization of the most recent influenza A(H5N1) viruses in both human and poultry populations, and serological investigations, are critical to assess associated risks to public health and promptly adjust risk management measures.
There are no specific vaccines for influenza A(H5N1) in humans. However, candidate vaccines to prevent influenza A(H5) infection in humans have been developed for pandemic preparedness in some countries. WHO continues to update the list of zoonotic influenza candidate vaccine viruses (CVV) twice a year at the WHO consultation on influenza virus vaccine composition. The list of such CVVs is available on WHO website. In addition, the genetic and antigenic characterizations of contemporary zoonotic influenza viruses are published on Global Influenza Programme (who.int).
WHO Advice
This event does not change the current WHO recommendations on public health measures and influenza surveillance.
Given reports of sporadic influenza A (H5N1) cases in humans, outbreaks in mammals, the widespread circulation in birds and the constantly evolving nature of influenza viruses, WHO continues to stress the importance of global surveillance to detect and monitor virological, epidemiological, and clinical changes associated with emerging or circulating influenza viruses that may affect human (or animal) health, and timely virus sharing for risk assessment.
The public should avoid high-risk environments, such as live animal markets/farms, and avoid contract with live poultry or surfaces that might be contaminated by birds or poultry droppings. Additionally, it is recommended to maintain good hand hygiene with frequent washing or use of alcohol- based hand sanitizer.
The general public and at-risk individuals should immediately report instances of sick animals or unexpected deaths in animals to veterinary authorities. Consumption of poultry that are sick or have died unexpectedly should be avoided.
In countries where avian influenza is known to cause outbreaks in poultry, people who handle live poultry for consumption should wear respiratory protection/barriers during slaughtering or when handling slaughtered poultry and should seek health care immediately if they feel unwell soon after such exposure.
Any person who has had exposure to potentially infected birds or contaminated environments and feels unwell should seek health care promptly and inform their healthcare provider of their exposure.
WHO advises against implementing any travel or trade restrictions based on the current information available on this event. WHO does not advise special traveler screening at points of entry or other restrictions due to the current situation of influenza viruses at the human-animal interface.
States Parties to the International Health Regulations (2005) are required to immediately notify WHO of any laboratory-confirmed case of a recent human infection caused by a new subtype of influenza virus. Evidence of illness is not required for this notification.
Further Information
- WHO Global influenza programme, human-animal interface
- WHO Monthly Risk Assessment Summary: Influenza at the human-animal interface
- WPRO Avian Influenza Weekly
- Protocol to investigate non-seasonal influenza and other emerging acute respiratory diseases:
- Summary of Key Information Practical to Countries Experiencing Outbreaks of A(H5N1) and Other Subtypes of Avian
- Maintaining surveillance of influenza and monitoring SARS-CoV-2 – adapting Global Influenza surveillance and Response System (GISRS) and sentinel systems during the COVID-19 pandemic
- Case definitions for the four diseases requiring notification in all circumstances under the International Health Regulations (2005)
- Evidence-based risk management along the livestock production and market chain: Cambodia
- Disease outbreak news Avian Influenza A (H5N1) Cambodia, 26 February 2023
- Disease outbreak news Avian Influenza A (H5N1) Cambodia, 29 November 2023
- Food and Agriculture Organization of the United Nations (FAO) – Animal Production and Health division (NSAH). FAO-NSAH Animal Health Threats Update. 11 October 2023.
- Avian Influenza and Lunar New Year festivities: vigilance and precautions
Citable reference: World Health Organization (8 February 2024). Disease Outbreak News; Avian Influenza A (H5N1) – Cambodia. Available at: http://www.who.int/emergencies/disease-outbreak-news/item/2024-DON501












{kind=link}