

“Changing the narrative on suicide”
Suicide is a major public health challenge, claiming the lives of more than 720 000 people every year. Each life lost has profound social, emotional, and economic consequences, deeply affecting families, friends, workplaces, and entire communities around the world.
The triennial theme for World Suicide Prevention Day (2024–2026) is “Changing the Narrative on Suicide”. This theme calls on us all to challenge harmful myths, reduce stigma, and foster open, compassionate conversations about suicide. It is about shifting from silence and misunderstanding to openness, empathy, and support — creating environments where people feel able to speak up and seek help.
Changing the narrative also means driving systemic change. It calls for suicide prevention and mental health to be a priority in public policy, urging governments and institutions to take action. This includes developing and implementing evidence-based strategies, improving access to quality care, and ensuring that those in distress receive the support they need.
World Suicide Prevention Day (WSPD) was established in 2003 by the International Association for Suicide Prevention in partnership with the World Health Organization. Each year, on 10 September, WSPD focuses global attention on suicide prevention, uniting communities, organizations, and governments with the shared belief that suicides are preventable.
Key facts
- More than 720 000 people die due to suicide every year.
- Suicide is the third leading cause of death among 15–29-year-olds.
- Seventy-three per cent of global suicides occur in low- and middle-income countries.
- The reasons for suicide are multi-faceted, influenced by social, cultural, biological, psychological, and environmental factors present across the life-course.
- For every suicide there are many more people who attempt suicide. A prior suicide attempt is an important risk factor for suicide in the general population.
Overview
Every year 727 000 people take their own life and there are many more people who make suicide attempts. Every suicide is a tragedy that affects families, communities and entire countries and has long-lasting effects on the people left behind. Suicide occurs throughout the lifespan and was the third leading cause of death among 15–29-year-olds globally in 2021.
Suicide does not just occur in high-income countries but is a global phenomenon in all regions of the world. In fact, close to three quarters (73%) of global suicides occurred in low- and middle-income countries in 2021.
Suicide is a serious public health problem that requires a public health response. With timely, evidence-based and often low-cost interventions, suicides can be prevented. For national responses to be effective, a comprehensive multisectoral suicide prevention strategy is needed.
Who is at risk?
The link between suicide and mental disorders (in particular, depression and alcohol use disorders) and a previous suicide attempt is well established in high-income countries. However, many suicides happen impulsively in moments of crisis with a breakdown in the ability to deal with life stresses, such as financial problems, relationship disputes, or chronic pain and illness.
In addition, experiencing conflict, disaster, violence, abuse or loss and a sense of isolation are strongly associated with suicidal behaviour. Suicide rates are also high among vulnerable groups who experience discrimination, such as refugees and migrants; indigenous peoples; lesbian, gay, bisexual, transgender, intersex (LGBTI) persons; and prisoners.
Prevention and control
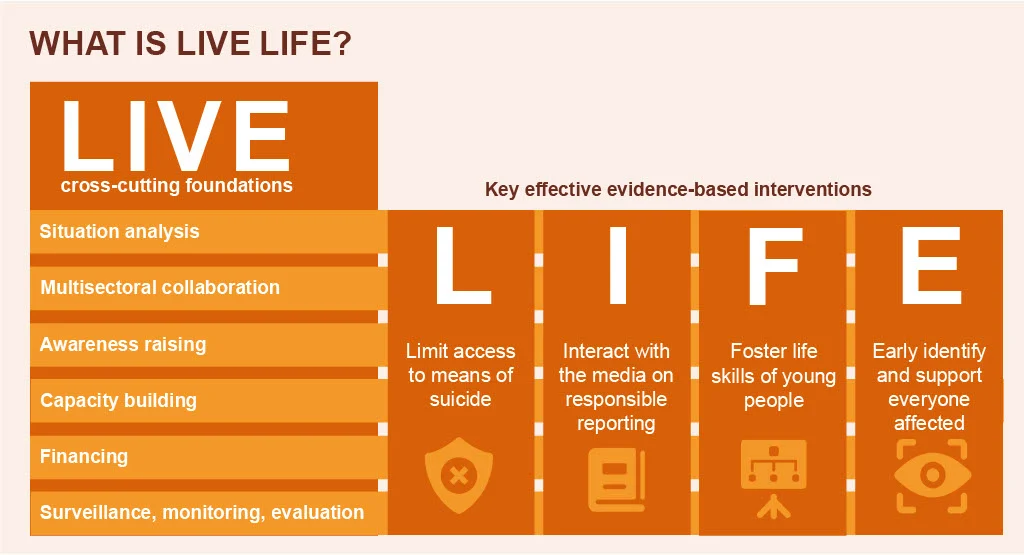
There are several measures that can be taken at population, sub-population and individual levels to prevent suicide and self-harm. LIVE LIFE, WHO’s initiative for suicide prevention, recommends the following key effective evidence-based interventions:
- limit access to the means of suicide (e.g. pesticides, firearms, certain medications);
- interact with the media for responsible reporting of suicide;
- foster socio-emotional life skills in adolescents; and
- early identify, assess, manage and follow up anyone who is affected by suicidal behaviours.
These need to go hand-in-hand with the following foundational pillars: situation analysis, multisectoral collaboration, awareness raising, capacity building, financing, surveillance and monitoring and evaluation.
Suicide prevention efforts require coordination and collaboration among multiple sectors of society, including the health sector and other sectors such as education, labour, agriculture, business, justice, law, defence, politics and the media. These efforts must be comprehensive and integrated given the multifaceted nature of suicide.
Challenges and obstacles
Stigma and taboo
Stigma, particularly surrounding mental disorders and suicide, means many people thinking of taking their own life or who have attempted suicide are not seeking help and are therefore not getting the help they need. The prevention of suicide has not been adequately addressed due to a lack of awareness of suicide as a major public health problem and the taboo in many societies to openly discuss it. To date, only a few countries have included suicide prevention among their health priorities and only 38 countries report having a national suicide prevention strategy.
Raising community awareness and breaking down the taboo is important for countries to make progress in preventing suicide.
Data quality
Globally, the availability and quality of data on suicide and self-harm is poor. Only some 80 WHO Member States have good-quality vital registration data that can be used directly to estimate suicide rates. This problem of poor-quality mortality data is not unique to suicide, but given the stigma surrounding suicide – and the illegality of suicidal behaviour in some countries – it is likely that under-reporting and misclassification are greater problems for suicide than for most other causes of death.
Improved surveillance and monitoring of suicide and self-harm are required for effective suicide prevention strategies. Cross-national differences in the patterns of suicide, and changes in the rates, characteristics and methods of suicide, highlight the need for each country to improve the comprehensiveness, quality and timeliness of their suicide-related data. This includes vital registration of suicide, hospital-based registries of self-harm and nationally representative surveys collecting information about self-reported self-harm.










{kind=link}