

Outbreak at a glance
As of 22 June 2022, 33 countries in five WHO Regions have reported 920 probable cases of severe acute hepatitis of unknown aetiology in children which fulfill the WHO case definition. Since the previous Disease Outbreak News published on 27 May 2022, 270 new probable cases have been reported to WHO, including from four new countries. This Disease Outbreak News includes updates on the epidemiology of the outbreak, the publication of the new interim guidance on laboratory testing, and the launch of the clinical case report form on the WHO Global Clinical Platform. The detection of severe acute hepatitis of unknown aetiology in children across five WHO Regions is unusual, and the severe clinical sequelae of some cases warrant detailed investigation.
Description of the outbreak
This outbreak was initially detected on 5 April 2022 when the United Kingdom of Great Britain and Northern Ireland (the United Kingdom) notified WHO of ten cases of severe acute hepatitis of unknown aetiology in previously healthy young children aged under 10 years in the central belt of Scotland.
As of 22 June 2022, 33 countries in five WHO Regions have reported 920 probable cases (Figure 1). These include new and retrospectively identified cases since 1 October 2021, which fit the WHO case definition as stated below. There are four additional countries that have reported cases which are pending classification and are not included in the cumulative probable case count. Of the probable cases, 45 (5%) children have required transplants, and 18 (2%) deaths have been reported to WHO.
Half of the probable reported cases have been reported from the WHO European Region (20 countries reporting 460 cases), including 267 cases (29% of global cases) from the United Kingdom (Table 1, Figure 2). The second highest number of probable cases have been reported from the Region of the Americas (n=383, including 305 cases from the United States of America), followed by the Western Pacific Region (n=61), the South-East Asia Region (n=14) and Eastern Mediterranean Region (n=2). Seventeen countries are reporting more than five probable cases. The actual number of cases may be underestimated, in part due to the limited enhanced surveillance schemes in place. The case count is expected to change as more information and verified data become available.
Figure 1. Distribution of probable cases of severe acute hepatitis of unknown aetiology in children by country, as of 22 June 2022 (n=920)

Table 1. Distribution of reported probable cases of severe acute hepatitis of unknown aetiologyby WHO Region since 1 October 2021, as of 22 June 2022
|
WHO Region |
Probable cases |
Cases requiring liver transplants |
SARS-CoV-2 positive by PCR (number of positive cases)
|
Adenovirus positive by PCR⸸ (number of positive cases) |
Adenovirus type 41 (number of positive cases) |
Deaths |
|
Americas |
383 |
23 |
11 |
118 |
14 |
12 |
|
Eastern Mediterranean |
2 |
0 |
Not available |
1 |
Not available |
1 |
|
Europe |
460 |
22 |
47 |
203 |
30 |
1 |
|
Southeast-Asia |
14 |
0 |
Not available |
Not available |
Not available |
4 |
|
Western Pacific |
61 |
0 |
6 |
5 |
0 |
0 |
|
Cumulative* |
920 |
45 |
64 |
327 |
44 |
18 |
*The information included in this table contains data notified under IHR (2005), including from The European Surveillance System (TESSY) and official sources detected through event-based surveillance activities within the Public Health Intelligence process. Further information is presented in the Annex table.
⸸ Adenovirus positive in any specimen type (respiratory, urine, stool, whole blood, serum, other, or unknown specimen type)
Laboratory testing of cases
Based on the working case definition for probable cases (Box 1), laboratory testing has excluded hepatitis A-E viruses in these children. Other pathogens were detected in a number of the cases, although the data reported to WHO are incomplete.
Adenovirus continues to be the most frequently detected pathogen among cases with available data. In the European region, adenovirus was detected by PCR in 55% of cases (203/371) with available results (see Annex). Preliminary reports from the United States indicate that adenovirus was detected in 45% of cases (113/252) with available results.
SARS-CoV-2 has been detected in a number of cases, however, data on serology results for are limited. In the European region, SARS-CoV-2 was detected by PCR in 15% of cases (47/307) with available results (see Annex). Preliminary reports from the United States indicate that SARS-CoV-2 was detected in 10% of cases (8/83) with available results.
For further details, please refer to the EURO/ECDC Joint surveillance report, the USCDC Technical Report, UKHSA Case Update and the UKHSA Third Technical Briefing.
Most reported cases did not appear to be epidemiologically linked; however, epidemiologically linked cases have been reported in Scotland, and the Netherlands.
Box 1. WHO Working case definition of acute hepatitis of unknown aetiology

Epidemiological characteristics of cases
Figure 2. Epidemiological curve of probable cases of severe acute hepatitis of unknown aetiology with available data, by week, by WHO region, as of 22 June 2022 (n=476)

Note: The figure only includes cases for which dates of symptom onset, hospitalization, or notification were reported to WHO (n= 476). The date of symptom onset was used when available (n=289). If unavailable, the week of hospitalization (n=163), or the week of notification (n=24), was used.
As of 22 June 2022, of 422 cases with information on gender and age, 48% of cases are male (n=202), and the majority of cases (78%, n=327) are under 6 years of age (Figure 3).
Figure 3. Age and gender distribution of reported probable cases of severe acute hepatitis of unknown aetiology with available data (n=422)
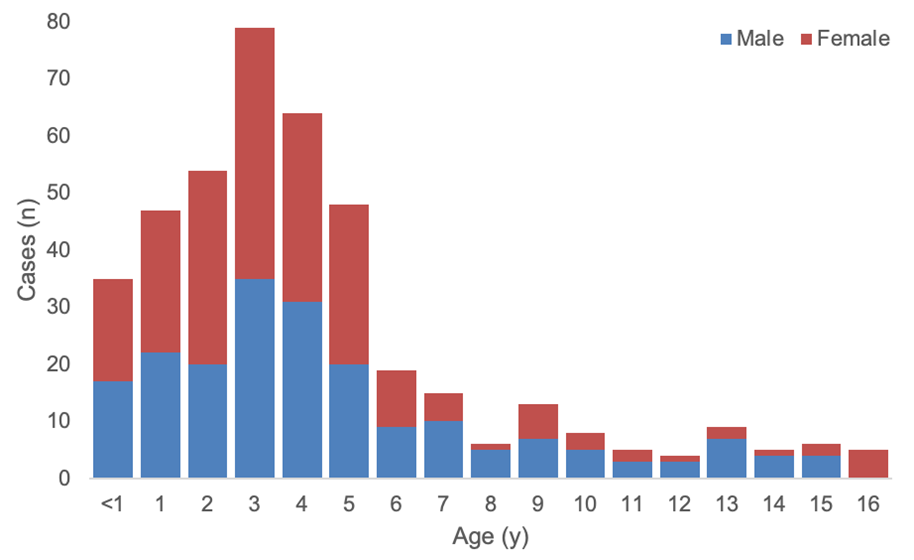
Out of 100 probable cases with available clinical data, the most commonly reported symptoms were nausea or vomiting (54% of cases), jaundice (49% of cases), general weakness (45% of cases) and abdominal pain (45% of cases).
Of all global cases, with available data, a total of 141 cases had both date of symptom onset and date of hospitalization available. Among these, the median number of days between date of symptom onset and date of hospitalization was four days [interquartile range (IQR) 7].
Public health response
WHO risk assessment
The risk at the global level is currently assessed as moderate considering the following factors:
- The aetiology of this severe acute hepatitis remains unknown and is being investigated;
- Limited epidemiological, laboratory, histopathological and clinical information are currently available to WHO;
- The actual number of cases and the geographical distribution may be underestimated, in part due to the limited enhanced surveillance schemes in place;
- The possible mode of transmission of the aetiologic agent(s) has not been determined;
- Although there are no available reports of healthcare-associated infections, human-to-human transmission cannot be ruled out as there have been a few reports of epidemiologically linked cases.
WHO advice
Laboratory testing
WHO has developed interim guidance for Member States on testing considerations and strategies for suspect cases of severe acute hepatitis of unknown aetiology in children. The guidance includes advice to support Member States with diagnostic prioritization and can be modified for regional considerations of endemic diseases. The guidance also considers assessments for other aetiological factors that are known to cause severe acute hepatitis in children, including other infectious agents, environmental exposures (toxins, medications), metabolic hereditary conditions, or autoimmune disorders, which should be considered in consultation with a paediatric hepatologist.
Prioritization should be given to routine collection of various specimens from as early after symptom onset as possible, to allow for later testing as required and to identify aetiology(ies). If laboratory capacity is limited, storage and referral to regional or global laboratories should be considered for the suggested investigative diagnostics. Any positive specimens should also be stored for further testing and/or investigation.
To further support Member States with laboratory testing, WHO is establishing a network of regional and global referral laboratories.
For more information, please see the Interim guidance on Laboratory testing for severe acute hepatitis of unknown aetiology in children.
Case reporting
WHO strongly encourages Member States to report cases of severe acute hepatitis of unknown aetiology in children matching WHO’s case definition, through established IHR mechanisms. For more information, please see the Suggested minimum variables for reporting cases of severe acute hepatitis of unknown aetiology in children.
Reporting clinical data through the WHO Global Clinical Platform
WHO has developed a clinical Case Report Form (CRF) to facilitate reporting of anonymized case-based data. The analysis of standardized global clinical data will contribute to understanding the aetiology as well as clinical characterization of disease, its natural history and severity; aiming to guide the public health response and the development of clinical management guidance including approaches to investigations and infection prevention and control interventions. WHO strongly encourages Member States’ participation in the WHO Global Clinical Platform for all cases meeting the WHO case definition, even if the CRF cannot be fully completed. Patient clinical data may be collected prospectively or retrospectively through examination and review of medical records.
The clinical CRF can be accessed through the WHO Global Clinical Platform for severe acute hepatitis of unknown aetiology.
Survey to estimate baseline incidence
Baseline data on the incidence of severe acute hepatitis of unknown aetiology from countries outside of the European Region remain scarce. Although voluntary, WHO encourages Member States to participate in the global survey by making aggregated data from different hospitals/centers across all regions, covering the last five years. This survey will help estimate baseline incidence, and importantly where cases are occurring at higher-than-expected rates.
Infection Prevention and Control
Until more is known about the aetiology of these cases, WHO advises implementation of general infection prevention and control practices including:
- Performing frequent hand hygiene, using soap and water or an alcohol-based hand-gel
- Avoiding crowded spaces and maintain a distance from others
- Ensuring good ventilation when indoors
- Wearing a well-fitted mask covering your mouth and nose when appropriate
- Covering coughs and sneezes
- Using safe water for drinking
- Following the Five Keys to Safer Food: (1) keep clean; (2) separate raw and cooked; (3) cook thoroughly; (4) keep food at safe temperatures; and (5) use safe water and raw materials.
- Regular cleaning of frequently touched surfaces
- Staying home when unwell and seeking medical attention
Health facilities should adhere to standard precautions and implement contact and droplet precautions for suspected or probable cases.
Annex table. Classification of reported probable cases of severe acute hepatitis of unknown aetiology by country since 1 October 2021, as of 22 June 2022
|
Country |
Probable/epi-linked cases* (cumulative 920) |
Cases requiring liver transplants (cumulative 45) |
SARS-CoV-2 positive by PCR (cumulative 64) (n/Number of cases tested if known)# |
Adenovirus positive by PCR (cumulative 327) (n/number of cases tested if known)⸸ |
Adenovirus type 41 (cumulative 44) (n/Number of cases tested unknown) |
|
Argentina |
3 |
1 |
0 |
2 |
1 |
|
Austria |
3 |
0 |
1 / 3 |
0 / 3 |
|
|
Belgium |
14 |
0 |
3 / 14 |
2 / 7 |
|
|
Brazil⸹ |
2 |
0 |
0 |
0 |
0 |
|
Bulgaria |
1 |
0 |
0 / 1 |
0 / 1 |
|
|
Canada |
12 |
2 |
3 / 10 |
2 / 10 |
0/1 |
|
Colombia⸹ |
2 |
0 |
0 |
1 |
0 |
|
Cyprus |
2 |
0 |
0 /1 |
1 / 2 |
0/1 |
|
Denmark |
7 |
|
|
0 / 7 |
|
|
France |
7 |
0 |
0 / 7 |
4 / 6 |
|
|
Greece |
11 |
0 |
0 / 8 |
2 / 9 |
|
|
Indonesia |
13 |
0 |
|
|
|
|
Ireland |
14 |
2 |
0 / 7 |
8 / 13 |
|
|
Israel |
5 |
|
0 / 2 |
1 / 2 |
|
|
Italy |
34 |
1 |
2 / 18 |
10 / 23 |
|
|
Japan |
58 |
0 |
5 |
4 |
0 |
|
Latvia⸹ |
1 |
0 |
|
1 / 1 |
|
|
Maldives |
1 |
0 |
|
|
|
|
Mexico |
58 |
0 |
|
|
|
|
Republic of Moldova |
1 |
0 |
0 / 1 |
0 / 1 |
|
|
Netherlands |
15 |
3 |
1 / 4 |
5 / 10 |
|
|
Norway |
5 |
0 |
2 / 5 |
2 / 5 |
2 |
|
Occupied Palestinian Territories |
1 |
0 |
|
|
|
|
Panama |
1 |
0 |
|
|
|
|
Poland |
8 |
0 |
0 / 2 |
2 / 5 |
|
|
Portugal |
15 |
0 |
|
|
|
|
Qatar⸹ |
1 |
|
|
1 |
|
|
Serbia |
1 |
1 awaiting |
0 / 1 |
1 / 1 |
|
|
Singapore |
3 |
0 |
1 |
1 |
0 |
|
Spain |
39 |
1 |
3 / 29 |
5 / 27 |
1 |
|
Sweden |
10 |
2, including 1 awaiting |
1 / 7 |
3 / 7 |
|
|
United Kingdom (the) |
267 |
12 |
34/196 |
156/241 |
27 / 35 |
|
United States of America |
305 |
20 |
8/83 |
113 / 252 |
13 / 20 |
Blank cells indicate where no data was available at the time of this report.
*The information included in this table contains data notified under IHR (2005), including from The European Surveillance System (TESSY) and official sources detected through event-based surveillance activities within the Public Health Intelligence process.
#All specimens with known test result (negative,or positive ) were included in the denominator.
⸸ Adenovirus positive in any specimen type (respiratory, urine, stool, whole blood, serum, other, or unknown specimen type) / number of cases with adenovirus test result in any specimen type. Any specimens with known test result (negative or positive) were included in the denominator.
⸹ Newly reported countries in this update
Further information
- Joint ECDC-WHO Regional Office for Europe Hepatitis of Unknown Origin in Children Surveillance Bulletin, 17 June 2022
- WHO minimum reporting variables for severe acute hepatitis of unknown aetiology in children
- WHO interim guidance on laboratory testing for severe acute hepatitis of unknown aetiology
- WHO minimum reporting variables line list template
- WHO Global Clinical Platform
- WHO Disease Outbreak News; Multi-Country – Acute, severe hepatitis of unknown origin in children (27 May 2022)
- The United Kingdom Health Security Agency (UKHSA) Acute Hepatitis Technical Briefing 3, (updated 19 May 2022)
- UKHSA case control study protocol (19 May 2022)
- Trends in Acute Hepatitis of Unspecified Etiology and Adenovirus Stool Testing Results in Children — United States, 2017–2022, Morbidity and Mortality Weekly Report (14 June 2022)
- United States Centers for Disease Control and Prevention Technical Report: Acute Hepatitis of Unknown Cause (16 June 2022)










{kind=link}