
Situation at a glance
Description of the situation
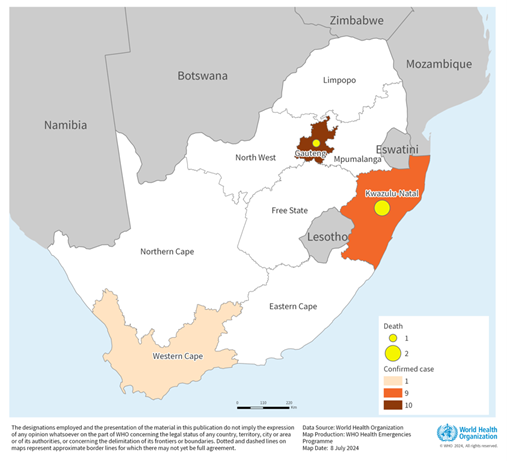
The IHR NFP of the Republic of South Africa notified WHO of 20 confirmed mpox (monkeypox) cases between 8 May and 2 July 2024, including three deaths (CFR 15%). These cases were reported in three of nine provinces: Gauteng (10 cases; 1 death), Western Cape (1 case), and KwaZulu-Natal (9 cases; 2 deaths).
The cases are all male, aged between 17 and 43 years, and almost all self-identified as men who have sex with men (MSM). Most are persons living with HIV, with unmanaged or only recently diagnosed HIV infection and advanced HIV disease (AHD), and one has diabetes. All cases were symptomatic, with extensive skin lesions and 18 required hospitalization. None of the confirmed cases reported a history of international travel and none reported attending high-risk social gatherings. The type of exposure reported by cases is sexual contact.
For the first 16 cases overall, 44 contacts were identified in KwaZulu-Natal, 39 contacts in Western Cape, and 55 in Gauteng province. While three of the four initial cases in KwaZulu-Natal were epidemiologically linked through contact tracing, at least the initial seven in Gauteng province were not found to be epidemiologically linked, suggesting community transmission is underway. Individual contact tracing for recent cases is ongoing. In addition, limited information suggests that some affected persons have attended and been exposed to mpox at parties or clubs where sexual activity occurs.
Genomic sequencing, available for five confirmed cases has identified sub-clade IIb MPXV, the clade linked to the multi-country mpox outbreak.
During the ongoing 2022-2024 multi-country outbreak, five mpox cases had previously been confirmed in South Africa, during the peak in June-August 2022, and all had reported travel abroad. None of the cases were severe. No cases were reported in 2023.
Figure 1. Geographic distribution of reported mpox cases and deaths, South Africa, 8 May to 2 July 2024 (n=20)

Epidemiology
Mpox is an infectious disease caused by the monkeypox virus (MPXV). There are two known clades of MPXV: clade I, previously called the Congo Basin clade; and clade II, previously called the West African clade, which includes subclades IIa and IIb. MPXV transmits between humans through close contact with lesions, body fluids, respiratory droplets or contaminated materials, or from animals to humans through contact with live animals or consumption of contaminated bushmeat. Mpox causes signs and symptoms which usually begin within a week of exposure but can start 1–21 days later. Symptoms typically last 2–4 weeks but may last longer in someone with a weakened immune system. Fever, muscle aches and sore throat appear first, followed by skin and mucosal rash. Lymphadenopathy (swollen lymph nodes) is also a typical feature of mpox, present in most cases. Children, pregnant women and people with weak immune systems are at risk of developing complications and death from mpox.
It is important to distinguish mpox from chickenpox, measles, bacterial skin infections, scabies, herpes, syphilis, other sexually transmissible infections, and medication-associated allergies. Someone with mpox may also concurrently have another sexually transmissible infection such as herpes. Alternatively, a child or adult with suspected mpox may have chickenpox. For these reasons, laboratory testing of skin specimens obtained by swabbing is important for confirmation of mpox, particularly for the first cases in an outbreak or new geographic area, and implementation of public health and social measures to curb transmission.
Treatment is based primarily on managing clinical symptoms, ensuring skin care, reducing pain, and preventing and managing complications. Where available through emergency or compassionate use programmes, specific antiviral medications such as tecovirimat can also be used in the treatment of mpox, particularly for severe cases or individuals at higher risk of complications.
Public health response
Coordination
- Establishment of a national mpox Incident Management Team (IMT), with biweekly multisectoral coordination meetings with provincial mpox response coordination.
- Mapping of implementing partners and non-governmental organizations at national, provincial, district and sub-district levels for coordination of response activities.
- Ministerial press briefing on mpox held on 12 June 2024.
- The National Department of Health issues regular mpox media statements emphasizing prevention measures and addressing stigma.
Surveillance
- Outbreak response teams deployed and supporting outbreak investigations.
- Ongoing contact tracing and active case search.
- Generation of weekly national mpox situation reports.
Laboratory:
- Mpox clinical specimen collection and processing guidelines updated and disseminated to health facilities.
- All public health facilities refer samples through the National Health Laboratory Service (NHLS) network to the National Institute for Communicable Disease (NICD) for testing.
- Private health facilities can test for mpox and send specimens for sequencing to the NICD.
- Target turnaround time for testing and reporting on results for suspected cases and symptomatic contacts is within 24 hours.
- Increasing testing capacity through decentralizing testing to include private laboratories.
- Preparations are underway to roll out mpox environmental surveillance leveraging established wastewater surveillance sites.
Case management:
- Implementation of immediate isolation of suspected and confirmed cases in a hospital or, for non-severe disease, at home, to prevent transmission.
- Fast tracking approval of national clinical guidelines and circulation to all public and private healthcare facilities.
- Ongoing capacity building for health and care workers, including a clinical management webinar attended by over 500 health professionals, to update clinicians on mpox case detection, clinical care, and infection prevention and control; provinces conducting training for healthcare workers.
- Supplemental clinical care, including mental health and psychological support for health workers, patients and their relatives prioritized for inclusion in case management guidelines, plans, and trainings.
- The Department of Health obtained authorization for use of tecovirimat from the South Africa Health Products Regulatory Authority (SAHPRA).
- Tecovirimat application through Section 21 (SAHPRA) and 15 courses of tecovirimat provided to South Africa by WHO.
Risk Communication and Community Engagement (RCCE):
- Messages developed to support risk communication and community engagement, which integrates aspects of sexual transmission of mpox.
- Risk communication messages translated into local languages and aligned with context.
- Sensitization of affected communities initiated in KwaZulu-Natal and Gauteng provinces; training for Health Promoters and other stakeholders conducted in Gauteng.
- Health promoters conducting health promotion talks at clinics and community settings on mpox as part of routine health promotion activities.
- Public awareness event at Braamfontein, Johannesburg conducted mid-June 2024, in conjunction with non-governmental organizations (NGOs).
- Engagement with relevant National Department of Health (NDoH) programmes to support RCCE activities (e.g., STI, HIV, TB etc.).
- Identified and engaged NGOs working with key populations (e.g., MSM).
- Partners engaged in awareness building during the Pride event in Durban.
- Regular online updates through the NICD webpage. Link
Vaccination strategies and research initiatives:
- National Advisory Group on Immunization (NAGI) Technical Working Group mpox vaccine recommendations for South Africa endorsed by the National Department of Health.
- Risk groups for pre-exposure vaccination include men who have sex with men, health workers and laboratory personnel while sexual, household, and health facility contacts will be offered post-exposure vaccination.
- Discussions are underway regarding options for vaccine procurement.
- WHO and partners supporting the development of vaccination strategies for emergency response and discussions regarding clinical vaccine studies for vaccines and therapeutics.
Infection Prevention and Control (IPC)
- Reviewing IPC action plans for health facilities and the community.
- Refresher training conducted for IPC staff.
- Guidelines on the safe management of human remains and burial updated and distributed, including training for undertakers.
Continuity of essential health services (CEHS)
- The affected provinces are conducting health facility readiness assessment to identify gaps.
- The mpox IMT is working to integrate prevention, screening and management of mpox into HIV and STI care in the Key Populations programme of the National Department of Health.
Equipment and resources:
- Logistics support was provided for the collection, transport, and examination of samples from suspected cases.
- Equity Pharma working with NDoH- Affordable Medicine Directorate (AMD) regarding access to therapeutics.
WHO risk assessment
The sudden appearance of unlinked cases of mpox in South Africa without a history of international travel, the high HIV prevalence among confirmed cases, and the high case fatality ratio suggest that community transmission is underway, and the cases detected to date represent a small proportion of all mpox cases that might be occurring in the community; it is unknown how long the virus may have been circulating. This may in part be due to the lack of early clinical recognition of an infection with which South Africa previously gained little experience during the ongoing global outbreak, potential pauci-symptomatic manifestation of the disease, or delays in care-seeking behaviour due to limited access to care or fear of stigma.
At present, most of the transmission in the initial cases is linked to recent sexual contacts among men, similar to the spread in newly affected countries during the 2022-2024 multi-country outbreak. For most confirmed cases, no epidemiological link has been established, possibly due in part to incomplete contact identification. This suggests that undetected community transmission is occurring and that further cases can be expected as surveillance is strengthened. The current risk to human health for the general public remains low in the country. The risk for gay men, bisexual men, other men who have sex with men, trans and gender diverse people, and sex workers is moderate, as currently assessed for the global outbreak. The higher risk assessment is consistent with ongoing transmission among recognized risk groups due mainly to exposure through sexual contact, and the higher prevalence of undetected or uncontrolled HIV infection in the country which also puts people at risk of severe disease. There is potential for increased health impact should wider dissemination continue in vulnerable groups in South Africa or neighbouring countries. Data from ongoing mpox outbreaks show that the risk of severe disease and death is higher among children, immunocompromised individuals including persons with poorly controlled HIV, and pregnant women.
The most recent Joint United Nations Programme on HIV/AIDS (UNAIDS) data estimate HIV prevalence among men who have sex with men in South Africa to be around 30%, only 44% of whom are on antiretroviral therapy. This makes this group extremely vulnerable to severe mpox disease and death. There is also a hazard to health workers if they are not appropriately using personal protective equipment (PPE) when caring for patients with mpox.
Prior to 2022, the CFR for clade II MPXV in West Africa was estimated to be 3.6% (95% CI: 1.7%, 6.8%). Case fatality in the ongoing multi-country outbreak (0.02%) is the lowest recorded for MPXV clade II. In contrast, the CFR among cases reported in South Africa in 2024 is extremely high (15%), as most detected cases are among persons who are immunocompromised with uncontrolled HIV and other co-morbidities. Persons with less severe mpox are less likely to recognize the condition or seek diagnosis and care; therefore, such cases may remain undetected and unreported.
Vaccination with mpox vaccines has been shown to be effective against mpox. The last case of smallpox in South Africa was reported in 1972, and smallpox vaccination stopped shortly after the global eradication of the disease in 1980. Thus, any immunity from prior smallpox vaccination (which is cross-protective for mpox) will at best now only be present in some persons over the age of 44 years. The median age of mpox cases in the current global outbreak is 34 years (IQR: 29 – 41) and within South Africa, reported cases are aged between 17-43 years.
The limited awareness of mpox and lack of knowledge about practices for prevention among health workers and among key populations such as sex workers or men who have sex with men in the country exacerbates their risk for mpox. Anyone suffering from disfiguring skin conditions, including mpox, may experience fear and stigma, which can be further compounded for key populations.
There is concern that the mpox outbreak in South Africa will continue to evolve given:
- The high likelihood of under-detection and under-reporting of local transmission, given that reported cases have to date almost exclusively affected the most vulnerable.
- Currently, all detected cases have presented with severe disease and extensive skin lesions, which could lead to more viral transmission and risks poor outcomes for the patients.
- While the government and partners are mobilized to introduce treatment for affected patients and vaccines for people at risk, these countermeasures are not yet widely available in the country.
- Public awareness of mpox and information about modes of transmission or possible amplifying events or risk of exposure in sex-on-premises venues remains limited in South Africa.
- Concurrent outbreaks of mpox are occurring in Africa and elsewhere, increasing the risk of further transmission.
WHO advice
General
Health authorities and clinicians/health and care workers of all countries should be aware that the global mpox outbreak linked to clade IIb MPXV is ongoing in all WHO regions and the risk of cross-border and international spread exists. National reporting to WHO is less complete and timely in recent months, and the number of cases continues to be underestimated globally.
WHO strongly advises that countries continue to follow the Standing Recommendations issued by the Director-General in August 2023, particularly concerning the epidemiological surveillance of mpox.
Countries should continue to strengthen the availability of and access to laboratory diagnostics in line with updated WHO interim guidance, including genomic sequencing of viruses. Detection of viral DNA by polymerase chain reaction (PCR) is the preferred laboratory test for mpox. The best diagnostic specimens are taken directly from the rash – skin, fluid or crusts – collected by vigorous swabbing. In the absence of skin lesions, testing can be done on oropharyngeal, anal or rectal swabs. However, while a positive result of oropharyngeal, anal or rectal sample confirms mpox, a negative result is not enough to rule out MPXV infection. Testing of blood is not recommended. Serology does not distinguish between different orthopoxviruses and is therefore restricted to reference laboratories where antibody detection methods may be applied for retrospective case classification or in special studies.
There must be sustained implementation of risk communication and community engagement appropriate to each context, maintenance or initiation of vaccination for persons at risk, optimal case management, adherence to infection control measures, strengthening research to better appreciate modes of transmission in different contexts, and sustained support for the development of rapid diagnostic methods and treatments adapted to the needs of patients.
Health authorities should strive to achieve the elimination of human-to-human transmission of mpox and ensure the maintenance of capacity for outbreak response. Anyone with a clinical or laboratory-confirmed diagnosis of mpox should follow the instructions of health authorities according to the local context, including isolation during the infectious period. Contacts of a confirmed case are asked to limit their movements (and advised to abstain from sexual relations) for 21 days, the monitoring period for the appearance of possible symptoms.
Vaccination against mpox is recommended for people possibly at risk of contracting the disease. Specific antiviral treatments are currently being assessed for efficacy against mpox, such as tecovirimat. Access to tecovirimat is possible through national application for use under the WHO MEURI protocol or request to WHO for access to the reserve for compassionate use.
It is essential to deepen knowledge in different contexts on optimal case management in the event of mpox and HIV co-infection, especially for patients who must initiate antiretroviral treatment.
In the community
Risk communication and community engagement activities are vital in motivating affected communities to become aware of the risks and protective behaviours, and to understand, prevent and combat stigma and discrimination. In this outbreak, there is continuing risk of exposure to mpox in the community through sexual activity in high-risk settings where multiple sexual contacts may occur.
Key audiences should be identified and advice provided to health professionals, community organizations, managers of events and sex-on-premises venues, key populations including commercial sex workers, men who have sex with men, trans and gender-diverse individuals, people working at or attending venues and events where sexual activity takes place, and people at risk of more serious illness (including persons living with untreated or poorly controlled HIV infection). To keep venues safe, a risk-based approach is recommended, including risk evaluation, risk mitigation and risk communication for personnel and clients, accompanied by rigorous environmental infection prevention and control practices.
Patients without severe disease who can isolate at home should be given advice on how to care for themselves. This includes advice for taking care of the rash (don’t scratch, clean your hands before and after touching lesions, keep your rash clean with sterilized water/antiseptic etc.) and supporting the patient’s mental health (keep hydrated, eat well, get enough sleep, use medication for pain and fever if needed, do things you find relaxing/enjoyable etc.) Mental health and psychosocial support are essential for patients with mpox in all settings regardless of context. The details on public health advice on recovering from mpox at home are accessible in this link.
Health and care workers who provide care to patients in the community and/or household settings should refer to WHO Interim Rapid Response Guidance on case management and infection prevention and control for mpox for guidance on the IPC measures recommended. It is vital that infection control measures be implemented to prevent and stop transmission of mpox in household and community settings that may amplify risk.
In healthcare settings
Implementing IPC measures in health care settings is necessary to prevent and stop the transmission of mpox. It is important to train staff on mpox and the appropriate control measures, such as standard and transmission-based precautions. Staff should also have access to and appropriately wear personal protective equipment, adhere to the WHO 5 Moments for hand hygiene, ensure frequent cleaning and disinfection of the patient environment, and implement appropriate patient placement and isolation. For further guidance on IPC measures required when caring for patients with mpox, please refer to WHO interim guidance Clinical Management and Infection Prevention and Control for monkeypox.
While protecting themselves with recommended measures, health and care workers should also ensure that stigmatization of patients with mpox is avoided and that psychological support is provided to patients and their families.
At points of entry
It is recommended to encourage authorities, health and care workers and community groups to provide travellers with relevant information to protect themselves and others before, during and after travel to events or gatherings where mpox may present a risk. WHO advises against any travel and trade restrictions based on available information on the current outbreak.
As not all viral genomes from these cases have yet been sequenced, and there is known extensive commercial and professional exchange between South Africa and central Africa, it is also critical to remain vigilant regarding the possibility of importation of clade I strains to South Africa.
Further information
- Standing recommendations for mpox issued by the Director-General of the World Health Organization (WHO) in accordance with the International Health Regulations (2005) (IHR); https://www.who.int/publications/m/item/standing-recommendations-for-mpox-issued-by-the-director-general-of-the-world-health-organization-(who)-in-accordance-with-the-international-health-regulations-(2005)-(ihr)
- WHO Strategic framework for enhancing prevention and control of mpox (2024-2027) : https://www.who.int/publications/i/item/9789240092907
- Risk communication and community engagement public health advice on understanding, preventing and addressing stigma and discrimination related to mpox; https://www.who.int/publications/m/item/communications-and-community-engagement-interim-guidance-on-using-inclusive-language-in-understanding–preventing-and-addressing-stigma-and-discrimination-related-to-monkeypox
- Public health advice for gay, bisexual and other men who have sex with men on the recent outbreak of mpox: https://www.who.int/publications/m/item/monkeypox-public-health-advice-for-men-who-have-sex-with-men
- Public health advice on mpox and congregate settings: settings in which people live, stay or work in proximity; https://www.who.int/publications/m/item/public-health-advice-on-mpox-and-congregate-settings–settings-in-which-people-live–stay-or-work-in-proximity
- Public health advice on mpox (monkeypox) and sex-on-premises venues and events; https://www.who.int/publications/m/item/public-health-advice-on-mpox-(monkeypox)-and-sex-on-premises-venues-and-events
- Public health advice for sex workers on mpox; https://www.who.int/publications/m/item/public-health-advice-for-sex-workers-on-monkeypox (disponible en français ici)
- Public advice on recovering from mpox (monkeypox) at home: https://www.who.int/news-room/public-advice/recovering-from-monkeypox-at-home#
- Clinical management and infection prevention and control for monkeypox: Interim rapid response guidance, 10 June 2022; https://www.who.int/publications/i/item/WHO-MPX-Clinical-and-IPC-2022.1
- 2022-24 Mpox (Monkeypox) Outbreak: Global Trends: https://worldhealthorg.shinyapps.io/mpx_global/ (link is external)
- Surveillance, case investigation and contact tracing for mpox: interim guidance, 20 March 2024: https://www.who.int/publications/i/item/WHO-MPX-Surveillance-2024.1
- Diagnostic testing for the monkeypox virus (MPXV): interim guidance, 10 May 2024
- https://iris.who.int/handle/10665/376952
- Meeting of the Strategic Advisory Group of Experts on Immunization, March 2024: conclusions and recommendations: https://www.who.int/publications/i/item/WER-9922-285-306
- WHO. Standard precautions for the prevention and control of infections: aide-memoires: https://www.who.int/publications/i/item/WHO-UHL-IHS-IPC-2022.1
Citable reference: World Health Organization (9 July 2024). Disease Outbreak News; Mpox (monkeypox) in South Africa. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2024-DON525










{kind=link}