
Situation at a Glance
Description of the Situation
From 1 January through 12 November 2023, a total of 12 569 suspected mpox cases, including 581 suspected mpox deaths (case fatality ratio: 4.6%), have been reported in 156 health zones from 22 out of 26 (85%) provinces in the Democratic Republic of the Congo. This is the highest number of annual cases ever reported, with new cases in geographic areas that had previously not reported mpox, including Kinshasa, Lualaba, and South Kivu. Among suspected cases, 1106 were tested by reverse transcriptase-polymerase chain reaction (RT-PCR), and 714 were positive for MPXV (positivity rate of 65%).
Cases with travel history to endemic provinces have been driving chains of human-to-human transmission in non-affected provinces (Figure 1 & 2).
Figure 1: Geographic distribution of suspected mpox cases by province, Democratic Republic of the Congo, 1 January – 4 November 2023 (Epi weeks 1 to 44) 
Figure 2: Geographic distribution of confirmed mpox cases by province, Democratic Republic of the Congo, 1 January – 7 October 2023 (epi weeks 1 to 40)

First cases of sexually transmitted clade I MPXV:
The first cluster of suspected cases of sexually transmitted mpox was identified in Kenge, Kwango province of the Democratic Republic of the Congo. It included six confirmed cases, five men and one woman, with no deaths among the confirmed cases. The first known case is a man, resident of Belgium with connections to the Democratic Republic of the Congo, who arrived in Kinshasa, on 15 March 2023 and started experiencing anal itching and discomfort the same day. On 16 March 2023, one day after arrival from Belgium, he travelled to the town of Kenge (260 km from Kinshasa). On 17 March, his anal lesion and genitals became painful blisters, and he developed further skin lesions on the trunk and buttocks. On 23 March, he consulted a doctor who suspected mpox, and a blood sample, oropharyngeal, rectal and vesicle swabs were performed on 24 March. The patient tested positive by RT-PCR of biological samples at the National Institute of Biomedical Research (INRB) in Kinshasa and the result was shared with the Ministry of Health on 10 April. Genomic sequencing of the sample confirmed that it was clade I MPXV.
The individual identified himself as a man who has sexual relations with other men. During his travel in the Democratic Republic of the Congo, he visited discretely operating known clubs of men who have sex with men and had several sexual contacts. He showed symptoms on the day of his arrival in the country, and with the mpox incubation period most often being more than one day, available information suggests that exposure took place outside the Democratic Republic of the Congo. Nonetheless, genetic analysis of the virus confirmed infection with a clade I strain, similar to other strains circulating in the Democratic Republic of the Congo. Although the patient had no reported exposure to another person with confirmed mpox, based on the epidemiological investigation exposure to mpox likely occurred in Belgium.
Epidemiological investigation following this first case identified several sexual and non-sexual contacts who were monitored over time for mpox signs and symptoms. Among 27 contacts identified and six tested, five sexual contacts tested positive for mpox: two were confirmed on 10 April and three on 18 April. Of these five contacts, three developed symptoms during their 21-day follow-up period. Two contacts who did not develop symptoms also tested positive by a mucous membrane sample. Of the five confirmed contact cases, four were men aged between 24 and 35 years old and one was a woman. The initial case confirmed having sexual contact with each of them. After his recovery from mpox he returned to Belgium on 5 May 2023.
This cluster of mpox cases represents the first documented sexual transmission of MPXV Clade I. It is also the first described transmission of MPXV Clade I among men who have sex with men. Notably, there are clubs in Kenge for men who have sex with men, some of whose members travel to visit other clubs within the country and outside the country, particularly in Europe and within Central Africa. In the city of Kinshasa, there are more than 50 such clubs. Some members of these clubs also reside outside the Democratic Republic of the Congo. This event is unusual and highlights the risk that MPXV clade I could also widely spread among sexual networks, as seen for clade II during the 2022-23 global outbreak.
On 28 July 2023, another confirmed case of mpox was recorded in another man who had sex with men in Kenge town in the Democratic Republic of the Congo. The patient was a man residing in Kenge, with onset of the disease on 11 June 2023. He was not listed among the contacts of the first group of cases and the limited epidemiological investigation did not directly link him to the March-April cluster. Genome sequencing for this case has not been performed. Further epidemiological investigations are being conducted to verify reports of new cases in this province.
First mpox outbreak in Kinshasa
In August 2023, for the first time, mpox cases were confirmed in Kinshasa, the capital of the Democratic Republic of the Congo. Four separate events were identified where persons exposed in other provinces (Equateur, Maindombe) travelled to Kinshasa, each leading to local transmission with small clusters in the capital. Between 18 August and 12 November 2023, a total of 102 suspected cases were reported in eight health zones in Kinshasa, including 18 confirmed cases with one confirmed mpox death (case fatality ratio of 5.6% among confirmed cases).
The first confirmed case was in a person who arrived from the Maindombe province, where mpox is endemic, to Kinshasa by river boat. He was confirmed on August 18 and subsequently several of his close contacts developed symptoms and tested positive for MPXV. Additional imported confirmed cases were reported in Limete, Makala and Nsele health zones. The sex ratio among confirmed cases in Kinshasa is men 2: women 1, with a median age of 24 (95% CI 11-27) years. For the moment, 13 of the confirmed cases have recovered (including a health worker), one died and four are isolated and under treatment. The person who died also had tuberculosis and acquired mpox during hospitalization, indicating nosocomial transmission.
These new reports of human-to-human transmission of mpox in a large urban area such as Kinshasa clearly illustrate that the epidemiology of mpox in the Democratic Republic of the Congo is changing.
First mpox outbreak in South Kivu
Before 2023, South Kivu province had not reported mpox. The first confirmed case was a young trader who travelled from Kisangani, in Tshopo province, one of the mpox endemic provinces, a few days before the onset of symptoms on 26 September 2023. The first skin lesions were located on his genitals and later extended to the whole body. During the initial epidemiological investigation, 113 contacts were registered in Bukavu and Kamituga health zones. As of 22 November 2023, a total of 80 suspected and 34 confirmed cases (including 20 sex workers) of mpox have been reported in South Kivu mainly from the Kamituga health zone, with no deaths. Currently South Kivu province is grappling with conflict, displacement, food insecurity, and challenges in providing adequate humanitarian assistance, all of which have a profound impact on the local population, especially vulnerable groups, and might represent fertile ground for further spread of mpox.
Animal studies
The natural reservoir of the monkeypox virus is unknown – various small mammals such as squirrels and monkeys can be infected, and non-human primates are known to be clinically susceptible. Over the decades, the Democratic Republic of the Congo and partners have carried out animal studies to better characterize the ecology of the virus and potential animal reservoirs or incidental hosts. Such studies have been carried out in the provinces of Equateur, Haut Uélé, Kwango, Kwilu, Maïndombe, Maniema, Sankuru, Sud Ubangi, Tshopo, and Tshuapa. Eco-epidemiolocal studies are ongoing with national and international research partners collaborating to determine reservoir and incidental hosts.
Epidemiology
Mpox (monkeypox) is an infectious disease caused by the monkeypox virus (MPXV). There are two known clades of MPXV: clade I, previously called the Congo Basin clade; and clade II, previously called the West Africa clade; clade II further has two subclades: clade IIa and clade IIb. The disease is caused by one of the two clades of MPXV transmitted between humans through close contact with lesions, body fluids, respiratory droplets or contaminated materials, or from animals to humans through contact with live animals or consumption of contaminated bushmeat.
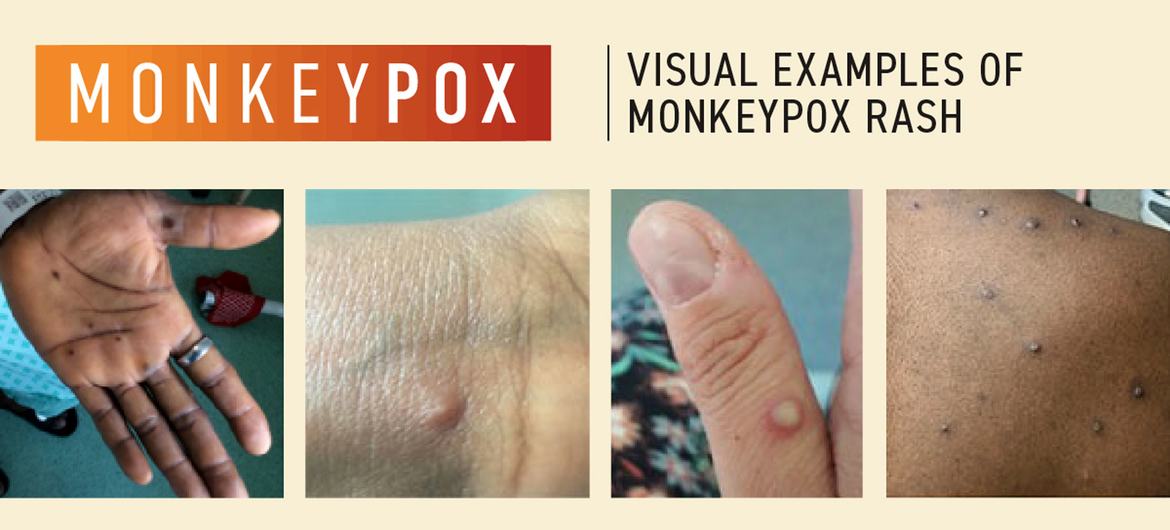
The incubation period ranges from two to 21 days, although some people can acquire infection without developing symptoms. Typically for mpox, fever, muscle aches and sore throat appear first, followed by skin and mucosal rash. Typically, the rash evolves over 2-4 weeks in stages – macules, papules, vesicles, pustules. Lesions dip in the centre before crusting over. Scabs then fall off. Lymphadenopathy (swollen lymph nodes) is also a typical feature of mpox, present in most cases. Children, pregnant people and people with weak immune systems are at risk for complications and death from mpox.
Identifying mpox can be difficult as other infections and conditions can look similar. It is important to distinguish mpox from chickenpox, measles, bacterial skin infections, scabies, herpes, syphilis, other sexually transmissible infections, and medication-associated allergies. Someone with mpox may also concurrently have another sexually transmissible infection such as herpes. Alternatively, a child or adult with suspected mpox may also have chickenpox. For these reasons, testing is key for people to get treatment as early as possible and to prevent further spread.
Detection of viral DNA by polymerase chain reaction (PCR) is the preferred laboratory test for mpox. The best diagnostic specimens are taken directly from the rash – skin, fluid or crusts – collected by vigorous swabbing. In the absence of skin lesions, testing can be done on oropharyngeal, anal or rectal swabs. However, while a positive result of oropharyngeal, anal or rectal sample is indicative of mpox, a negative result is not enough to exclude MPXV infection. Testing of blood is not recommended. Antibody detection methods may be used for retrospective case classification, but not diagnosis. It needs to be restricted to reference laboratories and it may not be useful as often it does not distinguish between different orthopoxviruses.
Treatment is based on taking care of the rash, managing pain, and preventing complications. In addition, specific antiviral medications such as tecovirimat can also be used in the treatment of mpox, particularly for severe cases or individuals at higher risk of complications. In the context of the global outbreak of mpox which began in 2022 (caused mostly by Clade IIb virus), the presentation of mpox varied, with some cases showing a rash appearing before or simultaneously with other symptoms, and the initial lesions were often localized on genitals and mucosae such as the mouth. For the first time the spread of MPXV has been driven and sustained by sexual contact among men who have sex with men who are members of large sexual networks.
Public Health Response
Emergency coordination:
- The Ministry of Public Health, Hygiene and Prevention prepared a budgeted national mpox preparedness and response plan.
- Further to this plan, an mpox Emergency Operations Centre and Incident Management Team were inaugurated in February 2023 to implement the following actions:
Monitoring and detection:
- Strengthening surveillance of mpox throughout the country and particularly in Kinshasa, Kenge and Kamituga.
- Distribution of sample collection and transport kits to reference hospitals and logistical support for collecting, transporting, and examining samples from suspected cases in Kenge, Kinshasa and other affected areas.
- Capacity building of health care providers and professionals in mpox surveillance, including detection of sexual transmission and other possible modes of transmission.
- Monitoring of contacts of clinical and laboratory-confirmed cases for a period of 21 days.
- Genetic sequencing of MPXV samples to better understand the circulating viral strain(s).
Communication and awareness:
- Information campaign on the risks of mpox and other sexually transmitted infections to groups potentially at risk, specifically targeting members of sex-clubs in Kenge and elsewhere.
- Identification and engagement of other clubs and populations potentially at risk.
- Establishment of a call center to facilitate alerts reporting and promote communication between health authorities and the communities concerned.
Case management and infection prevention and control:
- Supply of personal protective equipment to health professionals in Kenge, Kinshasa, Kamituga Maindombe and Tshopo.
- Isolation of confirmed cases in hospital or at home to prevent further transmission.
- Adapted clinical care, including psychological support, for persons with mpox.
Training and capacity:
- Training of laboratory workers from Kamituga, Kenge, Kinshasa and any other affected city or province on the collection, conservation, and appropriate delivery of mpox samples.
- Raising awareness among health authorities and health care providers across the country about mpox and its management.
WHO Risk Assessment
From 1 January to 12 November 2023, there has been a two-fold increase in the number of suspected mpox cases with 12 569 suspected cases reported, compared to 6216 in 2020, the highest annual number previously reported. Mpox has also been reported in new geographic areas such as Kinshasa, Kwango province and South Kivu. The reasons for this expansion, affecting men, women and children, remain unknown. Although increased awareness of the global mpox epidemic due to clade IIb MPXV has helped improve surveillance in the country, many aspects of the current situation remain to be elucidated.
Transmission of mpox through sexual contact enables faster spread from one person to another due to direct contact of mucous membranes, possibly leading to a shorter average incubation period. Immunocompromised individuals, either due to uncontrolled HIV or other immunocompromising conditions, are at higher risk for severe mpox complications and mpox-related death. While national HIV prevalence in the Democratic Republic of the Congo is estimated to be <1%, it is estimated to be 7.1% among men who have sex with men. Overall, an estimated 17% of people living with HIV in the country do not know their status, putting them at risk of developing advanced HIV infection, compromised immunity, and severe mpox disease.
The detection of clade I MPXV among visitors to a club of men who have sex with men in Kenge, some of whose members travel to visit other clubs within and outside the country, particularly in central Africa and in Europe, represents a risk for men who have sex with men in the Democratic Republic of the Congo and internationally. In the city of Kinshasa, it is estimated that there are over 50 similar clubs, and some of their members reside outside the Democratic Republic of the Congo.
It is still unclear what proportion of mpox cases in the Democratic Republic of the Congo may be exposed through sexual contact; however, with outbreaks linked to sexual transmission documented in 2023 in three previously unaffected provinces, the potential additional public health impact of this new observation could be significant, particularly in under-resourced urban areas. The rapid evolution of the new outbreak in South Kivu, including among sex workers, is also concerning.
Additionally, the first case identified in Kinshasa had traveled to the city by boat on the Congo river. These boats constitute a potentially high exposure environment since people are often in proximity, transporting animals, selling and consuming wild game on board, and often traveling on the boats for weeks while sharing beds and sometimes engaging in sexual activities. Moreover, the human-to-human spread potential is amplified in urban settings such as Kinshasa and the implementation of containment measures is more challenging.
Response capacities for mpox remain limited in the country. Surveillance and laboratory capacities remain suboptimal: only 9% (1106 / 12 569, as of week 44) of suspected cases this year have been tested by PCR. There are no immunization programmes for populations at risk of mpox in the Democratic Republic of the Congo outside of research projects, and access to the antiviral medication tecovirimat also remains limited to a few clinical research studies in the country.
Risk communication and community engagement are therefore of critical importance to address the risk posed by modes of transmission traditionally reported as bushmeat consumption and community outbreaks, as well as for the newly described risk of sexual transmission, particularly among men who have sex with men. According to a recent WHO study, awareness of the risks associated with mpox is low in the Democratic Republic of the Congo. Additionally, anyone suffering from disfiguring skin conditions, including due to mpox, may face stigma, and the lack of health messages to date for men who have sex with men in the country exposes this population to a particular risk.
In summary, the reasons for concern about further spread of mpox in the Democratic Republic of the Congo are as follows:
- The Democratic Republic of the Congo is experiencing a significant increase in the number of suspected cases reported in 2023;
- Geographic expansion of the presence of mpox is underway in the newly affected southern and eastern provinces of the country;
- Epidemiological and scientific knowledge about mpox remains limited and modes of transmission in the country are poorly understood;
- In 2023, confirmed cases of mpox have been reported in the large urban area of Kinshasa and several other previously unaffected areas for the first time;
- Sexual transmission of mpox due to clade I MPXV is being documented for the first time and chains of transmission may have been missed;
- Key populations experience a higher prevalence of HIV infection than the general population;
- Awareness of mpox and the associated risks are insufficient in the general and key populations;
- National response capacities face challenges, including limited epidemiological information on exposure and infection risk factors, limited public awareness of mpox and prevention measures, and numerous competing priorities;
- Collaboration and coordination among partners are needed to sustain essential research and support a robust response at national as well as provincial and local levels.
The risk of mpox further spreading to neighbouring countries and worldwide appears to be significant. In addition to the features outlined above, arguments supporting the assessment of a high risk of international spread of mpox include the following:
- These first reported outbreaks of mpox due to clade I MPXV linked to sexual contact include a history of international travel within and across WHO regions;
- The introduction of clade I MPXV in different and possibly intersecting sexual networks could facilitate and amplify the spread of this historically more virulent clade of the virus;
- A concurrent outbreak of mpox is occurring in the neighbouring Republic of Congo along the Congo River ecosystem, whose links, if any, with cases in the Democratic Republic of the Congo remain unknown.
These factors pose an additional risk of mpox outbreaks with potentially more severe consequences than the one which has been affecting the world since 2022.
WHO Advice
All countries, including their health authorities and clinicians/healthcare workers, should take note that the global mpox outbreak is ongoing; and, furthermore, the occurrence of sexual transmission of the clade I virus has been confirmed. Infection with clade I MPXV may lead to an increased risk of severe illness.
It is therefore strongly advised that countries continue to follow the Standing Recommendations of the Director-General of the WHO issued in August 2023, particularly concerning the epidemiological surveillance of mpox, strengthening of laboratory diagnostic capacities and genomic sequencing of viruses, community engagement and risk communication, making vaccines available, optimal case management, strengthening research to better understand modes of transmission in different contexts, and sustained support for the development of rapid diagnostic methods and treatments tailored to the needs of patients.
In all settings, it is essential to emphasize the importance of case investigation with sensitivity and absence of stigma and in-depth understanding of human-to-human transmission of mpox in communities, while strengthening the One Health approach in areas where the monkeypox virus circulates in possible mammalian hosts or reservoirs.
It is essential to deepen knowledge in different contexts about the links between mpox and HIV infection, their respective and common risk factors, to provide a population specific health service, and to integrate surveillance and case management within a strengthened and agile health service which meets patient needs.
Actions in the community
Communication on the risks of sexual transmission of mpox must be strengthened, especially among the people most at risk and individuals and households affected by this disease. Advocacy must be done at all levels to support, inform and engage community leaders in implementing the necessary measures to inform and engage their communities about mpox and how to stop its spread.
Risk communication and community engagement activities will be vital in motivating affected communities to become aware of the risks and locally relevant protective behaviours. Socio-behavioural data should be collected, and a situation analysis should be carried out to better understand transmission and risk factors. This information can then be used to improve decision-making, to ensure response efforts are aligned with community needs, priorities and capacities, and to inform the development of risk communications plans and evidence-based community engagement. Key audiences should be identified, including health professionals, men who have sex with men, people working at or attending venues and events where sexual activity takes place, sex workers, and people at risk of more serious illness (including those whose HIV is not treated or adequately controlled).
Partnerships should be established with trusted networks working with these communities to facilitate community engagement. Two-way feedback systems should be established or activated. Particular attention should be paid to measures to understand, prevent and combat stigma and discrimination – these are never acceptable and can undermine the response to the epidemic and have a serious impact on health outcomes.
Concerning the health facility, points of entry and control
Infection prevention and control measures in community venues and health centers are necessary to prevent and respond to outbreaks of mpox. It is important to train staff on the risks linked to contamination, to provide protective equipment, hand washing and hygiene devices in hospitals and at entry/control points; and ensuring appropriate patient isolation is in place. Health care professionals caring for patients with suspected or confirmed mpox infection should take “standard,” “contact,” and “droplet” precautions.
While protecting themselves with recommended measures, healthcare workers should also ensure that stigmatization of patients with mpox is avoided, and that psychological support is provided to patients and their families.
WHO advises against any travel or trade restrictions for the current outbreak.
When collecting clinical and laboratory specimens
Specimens collected from persons and animals suspected of being infected with MPXV should be handled by trained personnel working in equipped laboratories. Confirmation of monkeypox virus depends on the type and quality of the sample, and the type of laboratory test. Thus, specimens must be packaged and shipped in accordance with national and international requirements. RT-PCR is the preferred laboratory test, given its accuracy and sensitivity. For this, the optimal diagnostic samples for MPXV should be taken from skin or mucosal lesions – fluid from vesicles and pustules, and dry scabs. PCR blood tests are generally inconclusive due to the short duration of viremia compared to the time of sample collection after the onset of symptoms; they should not be systematically collected from patients. Because orthopoxviruses are serologically cross-reactive, antigen and antibody detection methods are not sufficiently specific for MPXV and do not constitute a formal confirmatory diagnosis. It is therefore essential that laboratories support health authorities in providing specimen collection kits for skin or mucosal lesions.
Preventive measures
Anyone with a clinical or laboratory-confirmed diagnosis of mpox should follow the instructions of health authorities according to the local context, including isolation during the infectious period whenever feasible. Contacts of a confirmed case should be monitored or should self-monitor for any sign or symptom, practice hand hygiene and respiratory etiquette, avoid contact with immunocompromised individuals, children, or pregnant women, and avoid sexual contact and non-essential travel for a period of 21 days from the last contact with a person with mpox.
Vaccines and antiviral treatments
Vaccines for the prevention of mpox are composed of vaccinia virus and were first developed as safer vaccines for the purpose of smallpox preparedness: third-generation vaccines causing fewer side effects than the vaccines used during smallpox eradication are available. These include MVA-BN, first approved for the prevention of mpox in 2019 and the LC16-KMB vaccine approved for mpox in 2022. These vaccines offer 66-90% protection against mpox due to the antigenic similarity of the viruses that cause smallpox and mpox. A few countries maintain stocks of vaccines against smallpox and mpox, especially since the start of the global outbreak in 2022. Vaccination against mpox is recommended for persons at risk of contracting the disease, including children, and persons who have been in close contact with someone who has mpox.
Antivirals are also being developed and a clinical trial of the antiviral agent tecovirimat is ongoing in the the Democratic Republic of the Congo in two district hospitals in the provinces of Maniema & Sankuru. In order to access tecovirimat in the country, a request can be made to national health authorities.
Further Information
WHO interim technical guidance:
- https://www.who.int/publications/i/item/who-mpx-laboratory-2023-1
- Surveillance, case investigation and contact tracing for mpox (monkeypox): interim guidance, 22 December 2022; https://www.who.int/publications/i/item/WHO-MPX-Surveillance-2022.4
- Vaccines and immunization for monkeypox: Interim guidance, 16 November 2022; https://www.who.int/publications/i/item/WHO-MPX-Immunization
- Clinical management and infection prevention and control for monkeypox: Interim rapid response guidance, 10 June 2022; https://www.who.int/publications/i/item/WHO-MPX-Clinical-and-IPC-2022.1
Surveillance and other data
- https://www.who.int/publications/m/item/monkeypox-minimum-dataset-case-reporting-form-(crf)
- 2022-23 Mpox (Monkeypox) Outbreak: Global Trends; https://worldhealthorg.shinyapps.io/mpx_global/
- UNAIDS. Democratic Republic of the Congo.; https://www.unaids.org/en/regionscountries/countries/democraticrepublicofthecongo
Risk communication and community engagement and Public Health Advice
- https://www.who.int/publications/i/item/WHO-MPX-RCCE-2022.1
- Risk communication and community engagement public health advice on understanding, preventing and addressing stigma and discrimination related to mpox; https://www.who.int/publications/m/item/communications-and-community-engagement-interim-guidance-on-using-inclusive-language-in-understanding–preventing-and-addressing-stigma-and-discrimination-related-to-monkeypox (disponible en français ici)
- Public health advice for sex workers on mpox; https://www.who.int/publications/m/item/public-health-advice-for-sex-workers-on-monkeypox (disponible en français ici)
- Public health advice on mpox and congregate settings: settings in which people live, stay or work in proximity; https://www.who.int/publications/m/item/public-health-advice-on-mpox-and-congregate-settings–settings-in-which-people-live–stay-or-work-in-proximity (disponible en français ici)
- Public health advice on mpox (monkeypox) and sex-on-premises venues and events; https://www.who.int/publications/m/item/public-health-advice-on-mpox-(monkeypox)-and-sex-on-premises-venues-and-events (disponible en français ici)
- Mpox Q&A: What you need to know about mpox; https://www.who.int/europe/news-room/questions-and-answers/item/mpox-q-a–what-you-need-to-know-about-mpox (disponible en français ici )
Strategic Planning and global support
- https://www.who.int/publications/i/item/WHO-Mpox-Outbreak_response-Ethics-2023.1
- Smallpox vaccines, SAGE September 2023: meeting highlights; https://www.who.int/publications/m/item/sage-september-2023–meeting-highlights
Citable reference: World Health Organization (23 November 2023). Disease Outbreak News; Mpox (monkeypox) in the Democratic Republic of the Congo. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON493









{kind=link}