
Situation at a glance
Sporadic cases of measles were reported in South Africa throughout 2022. In epidemiological week 40 in 2022 (ending 8 October 2022) an outbreak was declared in Limpopo province. As of 16 March 2023, confirmed cases have been reported from all provinces; eight out of nine South African provinces have declared measles outbreaks1. No deaths associated with measles have been recorded. Most cases (86%) are reported among those aged under 14 years.
Community-based surveillance has been strengthened and the Ministry of Health (MoH) is conducting a mass measles vaccination campaign targeting children aged between 6 months and 15 years in all provinces.
WHO assesses the risk posed by the current outbreak as high at the national level, moderate at the regional level and low at the global level.
Description of the situation
South Africa is a measles-endemic country, with several measles outbreaks reported in recent years.
Sporadic cases were reported in all nine provinces in South Africa in 2022. As of 4 March 2023, measles outbreaks were declared in eight provinces, further to the outbreak which was declared in Limpopo province in October 2022 (Figure 1).
Figure 1: Epidemiological curve of laboratory-confirmed measles cases in South Africa from week 40, 2022 to week 10, 2023 Source: NICD South African Measles Outbreak 2023 Update 16 March

From epidemiological week 40, 2022 (ending 8 October 2022) to week 10, 2023 (ending 7 March 2023), the National Institute of Communicable Diseases (NICD) tested 4830 serum samples for measles, of which 772 (16%) were confirmed measles cases (Figure 2).
Figure 2: Number of serum samples tested by NICD and positivity rate (%) in South Africa, week 40 of 2022 to week 10 of 2023

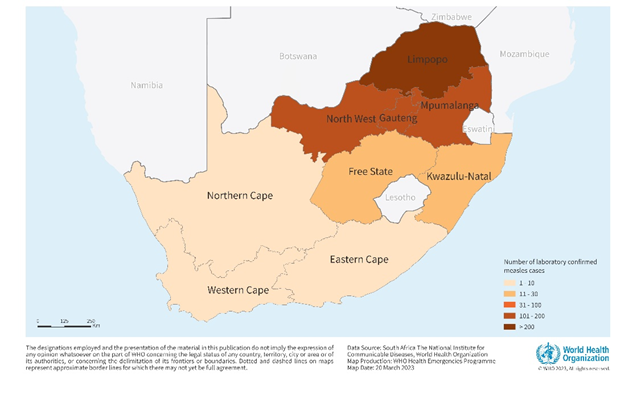
The 772 laboratory-confirmed measles cases were reported from the provinces of: Limpopo (275; 36%), North West (198; 26%), Gauteng (124; 16%), Mpumalanga (106; 14%), Free State (28; 3.5%), KwaZulu-Natal (17; 2%), Western Cape (11; 1.5%), Northern Cape (7; 1%) and Eastern Cape (6; 1%) (Figure 3).
Figure 3: Geographical distribution of laboratory-confirmed measles cases in South Africa, week 40 of 2022 (ending 8 October 2022) to week 10 of 2023 (ending 4 March 2023)

The age of laboratory-confirmed measles cases ranges from two months to 60 years. The majority of cases (42%) are in the age group 5-9 years, followed by the age groups 1-4 years (25%) and 10-14 years (19%). The attack rates (per 100 000 population) are highest among age groups 1-4 years (4.7 / 100 000) and 5-9 years (6.6 / 100 000).
Out of the laboratory-confirmed cases, 80 (10%) were vaccinated with at least one dose of measles-containing vaccine (MCV), 92 (12%) were unvaccinated, and the vaccination status of 570 (79.1%) is unknown.
According to the South African National Department of Health (NDOH), national immunization coverage of the measles-containing vaccine first dose (MCV1) and second dose (MCV2) was estimated at 87% and 82% respectively in 2021, while in 2022 the respective coverage was 86% and 86%. However, historical vaccination coverage has been low, which may be contributing to the current resurgence. According to WHO-UNICEF estimates, in 2018, MCV1 coverage averaged 81% and MCV2 75%. In 2017, MCV1 and MCV2 coverage was estimated at 81% and 78%.
Epidemiology of measles
Measles is caused by a virus in the paramyxovirus family. The virus infects the respiratory tract, then spreads throughout the body. Measles is a human disease and is not known to occur in animals. It can lead to major epidemics with significant morbidity and mortality, especially among vulnerable people. Among young and malnourished children, pregnant women and immunocompromised individuals, including those with HIV, cancer or treated with immunosuppressives, measles can cause serious complications, including ear infection, severe diarrhea, blindness, encephalitis, pneumonia, and death.
Transmission is primarily person-to-person by airborne respiratory droplets that disperse rapidly when an infected person coughs or sneezes. Transmission can also occur through direct contact with infected secretions. Transmission from asymptomatic exposed immune persons has not been demonstrated. The virus remains active and contagious in the air or on infected surfaces for up to two hours. A patient is infectious from four days before the start of the rash to four days after its appearance. There is no specific antiviral treatment for measles and most people recover within 2-3 weeks.
An effective and safe vaccine is available for prevention and control. The measles-containing vaccine first dose (MCV1) is given at the age of nine months, while the second dose of the measles-containing second dose (MCV2) is given at the age of 15 months. A 95% population coverage of MCV1 and MCV2 is required to stop measles circulation.
In areas with low vaccination coverage, epidemics typically occur every two to three years and usually last between two and three months, although their duration varies according to population size, crowding, and the population’s immunity status.
South Africa has had several outbreaks in recent years. Between 2003 and 2005, an outbreak occurred with 1676 cases reported. In 2009-2010, a large outbreak occurred with 18 431 documented cases. In 2017, a small outbreak was declared in Western Cape, Gauteng, and Kwazulu-Natal provinces, with a total of 186 cases. In 2019, a cluster of measles cases was reported in Cape Town affecting four siblings with a travel history to a measles-affected country.
Public health response
The Ministry of Health has implemented the costed national measles response plan with the support of WHO. The NDOH is conducting a mass measles vaccination campaign in all provinces, targeting children aged 6 months – 15 years. WHO staff have been deployed to support all aspects of the response: coordination; information management and surveillance; case management; supplies and logistics; and risk communication and community engagement.
Other response activities include:
- Active case search, investigation and line listing of fever and rash cases;
- Weekly measles incident management support team (IMST) meeting conducted with all provinces;
- Weekly interim situation reports based on the results of laboratory tests being issued by the NDOH and NICD;
- Deployment of provincial and district rapid response teams (RRTs) to affected neighbourhoods;
- Training in preparation for the national immunization campaign, completed in all provinces;
- A local vaccination campaign targeting children aged 6 months to 5 years, conducted in Limpopo province;
- Training health workers on measles case identification and supportive case management to prevent measles complications and mortality
- Strengthening of community-based surveillance for early detection of cases using community health volunteers, with support from WHO;
- Raising community awareness via community health workers;
- Mapping of partners and resources to support the outbreak response, supported by WHO and partners.
WHO risk assessment
Four of the provinces affected by the current outbreak (Limpopo, Mpumalanga, Northwest, and KwaZulu-Natal) border Zimbabwe, Botswana and Mozambique. The cross-border movement of populations across the Southern African Development Community (SADC) region2 and the weak disease surveillance health systems in many SADC countries pose a threat for further international spread.
There is an ongoing measles outbreak in neighboring Zimbabwe. Response capacities in the region are also constrained due to the concurrent readiness and response efforts to COVID-19, cholera, mpox, wild poliovirus, floods and cyclones.
Based on the currently available information, the overall risk of measles in South Africa is assessed as high for the following reasons:
- The current measles outbreak has been declared in eight out of nine provinces, and cases have been confirmed in all provinces, with further spread likely due to a highly mobile population;
- The 2022 measles risk assessment reported 86% of districts as having medium to high risk for measles, based on the WHO measles risk assessment tool;
- Suboptimal national measles vaccination coverage (in 2022, the coverage was 86% for both MCV1 and MCV2, which is below the required coverage of 95% to achieve population herd immunity and thus prevent sustained transmission);
- The presence of high rates of HIV/AIDS and TB, which can worsen the clinical picture of measles, in the South African population;
- Floods reported in seven provinces, which have rendered sections of the population inaccessible during the ongoing measles vaccination campaign;
- The need for technical and logistical support to provinces, as most essential services and programs (including immunization) were impacted by the COVID-19 pandemic and are only now recovering from its devastating impact.
WHO advice
Although measles is highly contagious, an effective and safe vaccine is available for prevention and control. MCV1 is given at the age of 9 months in countries with both ongoing transmission and a high risk of measles mortality among infants. These countries should administer the routine MCV2 at the age of 15-18 months. However, in South Africa, MCV1 is given at 6 months and MCV2 is given at 12 months3. A 95% population coverage of MCV1 and MCV2 is required to stop measles circulation. Reaching all children with two doses of the measles vaccine is recommended to ensure immunity and prevent outbreaks, as about 15% of vaccinated children fail to develop immunity from the first dose.
Routine vaccination of children against measles, combined with mass immunization campaigns in countries with high morbidity and mortality rates, are key public health strategies to reduce burden and transmission.
There is no specific treatment for measles. Case management of measles focuses on supportive care as well as the prevention and treatment of measles complications and secondary infections. Since measles is highly contagious, patient isolation is an important intervention to prevent the further spread of the virus.
Oral rehydration salts should be used as needed to prevent dehydration. All children diagnosed with measles should receive two doses of vitamin A oral supplements, given 24 hours apart, irrespective of the timing of previous doses of vitamin A; 50 000 international units (IU) should be given to infants aged < 6 months, 100 000 IU to infants aged 6-11 months and 200 000 IU to children aged 12 months. This treatment restores low vitamin A levels in acute measles cases that occur even in well-nourished children, and can help prevent eye damage and blindness. Vitamin A supplements have also been shown to reduce the number of measles deaths.
Nutritional support is recommended to reduce the risk of malnutrition due to diarrhoea, vomiting and poor appetite associated with measles. Breastfeeding should be encouraged where appropriate.
In unimmunized or insufficiently immunized individuals, the measles vaccine may be administered within 72 hours of exposure to the measles virus to protect against disease. If the disease does subsequently develop, symptoms are usually less severe, and the duration of illness may be shortened.
WHO does not recommend any restrictions on travel or trade to or from South Africa.
Further information
- South Africa Institute for Communicable Disease: South African measles outbreak update 2023
- South Africa. Mid-Year Population Estimates 2021
- Hong H, Makhathini L, Mashele M, Malfeld S, Motsamai T, Sikhosana L. Annual measles and rubella surveillance review, South Africa, 2017. Natl Inst Commun Dis Public Heal Surveill Bull. 2017; 16 (2):64-77.
- Hong H, Makhathini L, Mashele M, Smit S, Malfeld S, Motsamai T, et al. Annual Measles, Rubella and congenital rubella surveillance review, South Africa, 2019.
- Annual measles, rubella and congenital rubella surveillance review, South Africa, 2019
- WHO Immunization dashboard
- WHO fact sheets on Measles
- Measles & Rubella Initiative
——————————————————
1. A confirmed measles outbreak is defined in Expanded Programme on Immunisation Diseases Surveillance Guide 3rd Edition (2015) as the occurrence of three or more confirmed measles cases (at least two of which should be laboratory- confirmed; IgM positive) in a health facility/ district/ sub-district (approximate catchment population of 100 000) in a month. The cases in Eastern Cape do not meet this outbreak definition.
2. The SADC is composed of 16 member states: https://www.sadc.int › member-states.
3. While seroconversion rates are lower when MCV is given at 6 months, countries can decide to start at 6 months if the risk of disease is very high in infants. The capacity to reach high MCV2 coverage at 12 months will determine whether the strategy is appropriate or not, the risk being that if MCV2 coverage is low, large cohorts of unimmunized children will progressively build up.
Citable reference: World Health Organization (21 March 2023). Disease Outbreak News; Measles – South Africa. Available at https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON446









{kind=link}