
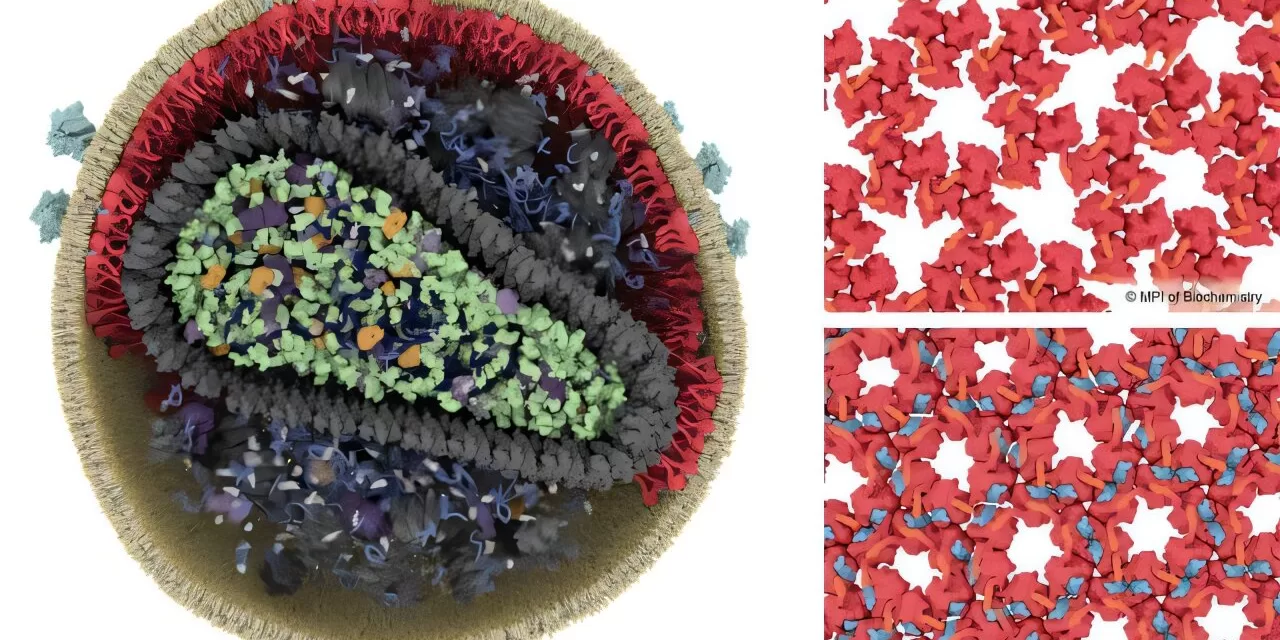
Recent research indicates that HIV-1 strains circulating in India are showing notable resistance to some of the world’s most potent broadly neutralising antibodies (bnAbs)—a discovery that may reshape strategies for HIV treatment and prevention in the country. The findings raise crucial questions about the adaptability of future therapies and the ongoing challenges in combatting a virus characterised by immense genetic diversity.
Key Findings: Indian HIV-1 Resistance Patterns
A peer-reviewed study published in Retrovirology and recent research in the Journal of Virology revealed that contemporary HIV-1 clade C strains, predominant in India, are significantly less responsive to several top bnAbs, including CAP256-VRC26.25, PGDM1400, and PGT121. The resistance patterns differ from those seen in the African subtype C strains. Notably:
-
V3 glycan-directed bnAbs (such as 10-1074 and BG18) and select CD4 binding site (CD4bs)-targeted bnAbs (e.g., VRC07, N6, 1-18) provide the best neutralisation in Indian strains, but with reduced potency compared to sensitive counterparts.
-
Resistance is associated with genetic changes in Env contact sites, variations in gp120 loop lengths, and different N-linked glycan profiles.
-
A predictive analysis suggests that only combinations of multiple bnAbs (rather than single therapies) could achieve near-complete neutralisation coverage for most Indian HIV-1 subtype C isolates.
-
Neutralisation resistance has trended upward in Indian populations between 2011 and 2016, hinting at evolving viral strategies against antibody therapies.
Expert Commentary: Implications and Next Steps
Dr. Sunil Solomon, an HIV researcher at YRGCARE (not involved in recent bnAb studies), remarks, “The resistance seen in Indian HIV-1 strains underscores the need to tailor therapies to local virus genetics. Multi-epitope bnAb cocktails may be preferable over single-antibody regimens, but further research is needed to optimise combinations and doses.”
Dr. Nandini Panneerselvam, lead author of a 2023 review on bnAbs, highlights, “As bnAbs move from laboratory to clinical trials, regional differences in HIV-1 genetics must inform both trial design and public health planning. The Indian case shows why a ‘one-size-fits-all’ approach can fail in diverse epidemics.”
Context and Background
Broadly neutralising antibodies have emerged over the past decade as promising adjuncts or alternatives to antiretroviral therapy (ART). Unlike standard ART, which suppresses viral replication, bnAbs are monoclonal antibodies that can bind to and neutralise a wide array of HIV-1 strains, preventing infection and controlling viremia. However, inducing robust bnAb responses via vaccination remains elusive, and the virus’s capacity for escape through mutation presents an ongoing obstacle.
India’s HIV epidemic is dominated by subtype C, known for rapid evolution and resistance development. As bnAbs progress toward clinical use, these Indian strain-specific resistance profiles may challenge the effectiveness and accessibility of cutting-edge therapies.
Statistical Context
-
India is home to the third-largest population of people living with HIV (PLHIV), with most (over 90%) infected by subtype C.
-
In a 2021 study, 71 full-length HIV-1 subtype C envs from Indian individuals were assessed for bnAb susceptibility, revealing wide variability in neutralisation profiles across antibodies and years.
-
Drug resistance mutations in ART-experienced patients run as high as 62.8%.
Practical Implications for Prevention and Treatment
For everyday health decisions, these insights carry several practical lessons:
-
ART remains the foundation for HIV control. Individuals should not expect bnAb therapies soon, but ongoing research may yield more effective options with regional tailoring.
-
Preventive vaccine development needs to account for genetic resistance markers—future vaccines that boost populations’ ability to generate multi-epitope bnAbs may be key.
-
Diagnostic screening for resistance mutations—though not yet widely available—may be needed to guide therapy choices and avoid ineffective interventions in high-resistance regions.
Limitations and Counterarguments
These studies should be interpreted with caution:
-
Sample sizes remain limited—broader surveys are needed to confirm region-wide resistance trends.
-
Longitudinal data is scarce; most resistance tracking is cross-sectional, limiting understanding of how mutations persist or evolve over time.
-
Multi-antibody combinations, while promising in predictive models, may face cost, logistics, and regulatory hurdles in real-world application.
Experts also caution against prematurely rethinking India’s HIV treatment protocols solely based on bnAb resistance data, as ART remains highly effective for the majority of cases.
Diverse Perspectives: The Role of Patient Experience and Public Health
Patient advocacy groups in India stress the importance of expanding access to current ART, improving routine resistance testing, and promoting public education about the challenges of viral mutation. Notably, vulnerable populations—such as people who inject drugs and men who have sex with men—may face higher risks of drug and antibody resistance, requiring targeted interventions.
Public health officials emphasise that integrating resistance research with national surveillance programs is crucial to optimising regimens and reducing HIV transmission.
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.
References







{kind=link}