
Situation at a Glance
Description of the Situation
On 30 January and 7 February 2024, the Bangladesh National Focal Point (NFP) for the International Health Regulations (IHR) notified the World Health Organization (WHO) of two epidemiologically unlinked cases of NiV infection.
First case confirmed on 21 January 2024
The first patient is a 38-year-old male from Manikganj district, Dhaka division. The patient developed a fever followed by respiratory distress, restlessness, and insomnia on 11 January 2024 and was admitted to a local hospital on 16 January. He was transferred to the intensive care unit of a hospital in Dhaka City on 18 January where he was intubated due to worsening of symptoms.
On 21 January, blood and throat samples were collected and the patient tested positive by reverse transcription polymerase chain reaction (RT-PCR) for NiV RNA from the throat sample and by enzyme-linked immunosorbent assay (ELISA) for anti-NiV Immunoglobulin M (IgM) from serum. On 27 January, the case was transferred to another hospital in Dhaka city, where he died on 28 January.
The case had a history of consuming raw date palm sap on 31 December 2023. As of 30 January 2024, a total of 91 contacts had been identified, including 11 family members, 20 from the community, and 60 healthcare personnel from different hospitals. However, none of the contacts tested positive for NiV by PCR or anti-NiV IgM by ELISA.
Second case confirmed on 31 January 2024
The second patient is a three-year-old female from Shariatpur district, Dhaka division. The patient visited a healthcare facility on 30 January 2024 with a two-day history of fever, altered consciousnesses, and seizures. The case was diagnosed with encephalitis and shock and was transferred to the isolation ward of another hospital in Dhaka city on the same day. Blood and throat samples were collected on 30 January and on 31 January, the case was laboratory-confirmed with NiV infection by RT-PCR for NiV RNA from the throat sample and by ELISA for anti-NiV IgM from serum and died on the same day.
The case had a history of regularly consuming fresh raw date palm sap. As of 7 February 2024, 67 contacts were identified, including three family members, 21 from the community and 46 healthcare personnel from different hospitals. All identified contacts tested negative for NiV by PCR or anti-NiV IgM by ELISA.
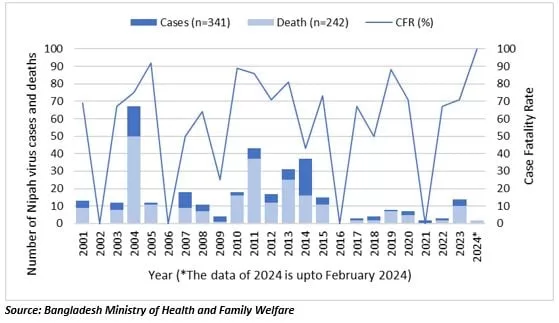
Since the report of the first case in 2001, human infections have been reported almost every year, with case fatality rate varying between 25% (in 2009) and 92% (in 2005) (Figure 1). Clusters of cases are mainly reported in the country’s central and northwest districts.
Figure 1. Number of reported Nipah virus cases and deaths by year, 1 January 2001 – 9 February 2024, Bangladesh.
Epidemiology
NiV infection is a bat-borne zoonotic disease transmitted to humans through infected animals (such as bats or pigs) or food contaminated with saliva, urine and excreta of infected animals. It can also be transmitted directly from person to person through close contact with an infected person (although less common). Fruit bats or flying foxes (Pteropus species) are the natural hosts for Nipah virus.
The incubation period is believed to range from 4 to 14 days. However, an incubation period of up to 45 days has been reported. Laboratory diagnosis of a patient with a clinical history of NiV infection can be made during the acute and convalescent phases of the disease by using a combination of tests. The main tests used are RT-PCR from bodily fluids and antibody detection via ELISA.
NiV infection in humans causes a range of clinical presentations including acute respiratory infection and fatal encephalitis. Further information about NiV infection can be found here.
The case-fatality rates in outbreaks across Bangladesh, India, Malaysia, and Singapore typically range from 40% to 100%, depending on local capabilities for early detection and clinical management. Although antivirals are in development, there are no licensed vaccines or therapeutics available for the prevention or treatment of NiV infection.
Public Health Response
The following public health response has been implemented by the government of Bangladesh and WHO:
- Nationwide awareness and health education activities are ongoing through print and electronic media, including distribution of posters and leaflets in the endemic districts.
- Risk communication activities engaging government officials, physicians, preachers, and farmers are ongoing. As of 31 January, these have been completed in Rajshahi, Jashore, Madaripur and Rajbari districts.
- WHO is working with the counterparts to strengthen surveillance, infection, prevention and control (IPC), risk communication, prompt diagnosis and management of infected patients.
- One Health Partners (Department of Livestock, Bangladesh Livestock Research Institute, Department of Forest, icddr,b) have been sensitized and engaged. Printed leaflets with health education messages have been produced.
WHO Risk Assessment
WHO assesses the overall risk at the national level to be moderate due to following reasons:
- The case fatality rate from NiV infection is high. Initial signs and symptoms of Nipah virus infection are non-specific, and the diagnosis is often not suspected at the time of presentation. This can hinder accurate diagnosis and creates challenges in outbreak detection, effective and timely infection control measures, and outbreak response activities.
- There are currently no specific drugs or vaccines available for NiV infection although WHO has identified Nipah as a priority disease for the WHO Research and Development Blueprint. Intensive supportive care is recommended to treat severe respiratory and neurologic complications.
- There is continued consumption of raw date palm sap by the community despite ongoing efforts for risk communication and community engagement to address food safety and risks to health.
- Despite these risk criteria, strong public health measures are in place to detect and control outbreaks including through the use of hospital-based systematic human NiV infection surveillance system which has been in place since 2006, and the utilization of the National Rapid Response Team (NRRT) at the central level and the Rapid Response Team (RRT) at the district level.
WHO assesses the risk at the regional level to be moderate. Although Bangladesh borders India and Myanmar, currently affected districts do not share an international land border. While there have not been any instances of cross-border transmission previously, this risk remains given the shared ecological corridor for the virus natural host (Pteropus bats) and occurrence among domestic animals and humans previously in both Bangladesh and India. India, however, has experience of controlling previous outbreaks of NiV infection.
WHO assesses the risk at the global level to be low, as there have been no previous confirmed cases outside Bangladesh, India, Malaysia, and Singapore.
WHO Advice
In the absence of a vaccine or licensed treatment available for Nipah virus disease, the key to reducing or preventing infection is by strengthening early detection surveillance and contact tracing, raising awareness of the risk factors and supporting people with measures they can take to reduce exposure to the NiV. Case management should focus on the delivery of timely supportive care and be supported by a good laboratory system. Intensive supportive care is recommended to treat severe respiratory and neurologic complications.
Public health educational messages should focus on:
- Reducing the risk of bat-to-human transmissionEfforts to prevent transmission should first focus on decreasing bat access to date palm sap and other fresh food products. Freshly collected date palm juice should be boiled, and fruits should be thoroughly washed and peeled before consumption. Fruits with signs of bat bites should be discarded. Areas where bats are known to roost should be avoided.
- Reducing the risk of animal-to-human transmissionNatural infection in animals has been described in farming pigs, horses, and domestic and feral cats. Gloves and other protective clothing should be worn while handling sick animals or their tissues, and during slaughtering and culling procedures. As much as possible, people should avoid being in contact with infected pigs. In endemic areas, when establishing new pig farms, considerations should be given to presence of fruit bats in the area and in general, pig feed and pig sheds should be protected against bats when feasible.
- Reducing the risk of human-to-human transmissionClose unprotected physical contact with NiV-infected people should be avoided. Regular hand washing should be carried out after caring for or visiting sick people.
- Controlling infection in health care settings
Health care workers caring for patients with suspected or confirmed infection, or handling their specimens, should implement standard infection control precautions at all times. As human-to-human transmission has been reported, particularly in health-care settings, contact and droplet precautions should be used along with standard precautions. Airborne precautions may be required in certain circumstances. Samples taken from people and animals with suspected NiV infection should be handled by trained staff working in suitably equipped laboratories.
WHO does not recommend any travel and/or trade restrictions toward Bangladesh based on the currently available information.
Further Information
-
- WHO South-East Asia Regional Strategy for the prevention and control of Nipah virus infection 2023-2030
- Nipah virus factsheet
- Situation Dashboard, Institute of Epidemiology, Disease Control and Research (IEDCR)
- Nipah Virus Transmission in Bangladesh
- Foodborne Transmission of Nipah Virus, Bangladesh
- Nipah Virus Disease: Epidemiological, Clinical, Diagnostic and Legislative Aspects of This Unpredictable Emerging Zoonosis
- The Ecology of Nipah Virus in Bangladesh: A Nexus of Land-Use Change and Opportunistic Feeding Behavior in Bats
Citable reference: World Health Organization (27 February 2024). Disease Outbreak News; Nipah virus infection – Bangladesh. Available at https://www.who.int/emergencies/disease-outbreak-news/item/2024-DON508









{kind=link}