
Jinka, Ethiopia – Ethiopia’s Ministry of Health reported on November 27, 2025, that the nation’s inaugural Marburg virus disease (MVD) outbreak has intensified, with confirmed cases reaching 12 and deaths climbing to eight. This marks a sharp rise from earlier figures, where six lab-confirmed cases and three deaths were noted as of November 20, prompting swift interventions by national authorities, the World Health Organization (WHO), and Africa CDC to curb spread in the South Ethiopia Region near the South Sudan border. The outbreak, centered in Jinka town of the Omo region, underscores vulnerabilities in fragile health systems amid concurrent crises like cholera and measles.
Outbreak Timeline and Current Status
The outbreak surfaced on November 12, 2025, when suspected viral hemorrhagic fever cases in Jinka prompted alerts from local health workers. Laboratory confirmation by the Ethiopian Public Health Institute (EPHI) on November 14 identified Marburg virus in patient samples from 33 tests, yielding six confirmed cases initially, including three deaths; three probable cases, all fatal, were epidemiologically linked but untested. By November 26, CDC data showed 12 lab-confirmed cases with seven deaths, updated to eight by November 27 per ministry reports, alongside two recoveries and two patients under treatment.
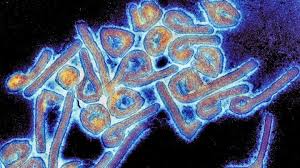
Contact tracing has identified over 206 individuals under active follow-up, with numbers fluctuating as investigations continue; earlier efforts isolated 129 contacts. Community screenings, isolation of cases, and hotline reporting are underway, supported by WHO teams enhancing surveillance, labs, and risk communication. Fruit bats, the natural reservoir like Rousettus aegyptiacus, are present in the area, though the infection source remains unidentified.
Understanding Marburg Virus Disease
Marburg virus disease, a filovirus akin to Ebola, causes severe hemorrhagic fever with an average case fatality rate of 50%, ranging 24-88% across outbreaks based on care access. Transmission starts from fruit bats to humans via direct contact with fluids or contaminated surfaces, then spreads person-to-person similarly. Initial symptoms mimic flu—high fever, headache, muscle pain, fatigue—progressing in 2-21 days (incubation) to rash, vomiting, diarrhea, abdominal pain, and bleeding from gums, nose, or orifices.
No approved vaccines or antivirals exist, though candidates advance in trials; treatment focuses on rehydration, symptom relief, and intensive care to boost survival. Past outbreaks hit Angola (2005, major), Uganda (2017-2018), Ghana (2022), Equatorial Guinea/Tanzania (2023), Rwanda (2024), and Tanzania (2025), all in sub-Saharan Africa. Ethiopia’s first event highlights rising frequency, possibly from deforestation increasing bat-human contact.
Response Strategies and Community Engagement
Ethiopia’s Ministry of Health leads with rapid response teams, emergency centers, and infographics in local languages detailing symptoms and prevention. Religious leaders, teachers, and congregation overseers pledged cooperation, vowing to educate believers on hand hygiene, avoiding bat handling/cooking, and isolating suspects—key since community buy-in halts chains. Africa CDC’s Jean Kaseya warned of risks to South Sudan and Kenya, integrating MVD response with mpox surveillance; WHO rates national risk high, regional moderate, global low.
Health Minister Mekdes Daba emphasized independent lab capacity at EPHI, urging symptom reporting without panic. “We have no active symptomatic cases under treatment currently, but vigilance is critical,” she noted in updates. Experts stress barrier nursing, PPE for providers, safe burials, and avoiding close contact with fluids.
Expert Insights and Public Health Implications
Dr. Elena Voss, WHO epidemiologist not involved in Ethiopia’s response, states: “Early detection and contact tracing, as seen here, can limit spread dramatically—fatality drops with prompt rehydration.” She highlights stretched resources from overlapping outbreaks straining Ethiopia’s system. Africa CDC integrates efforts to prevent cross-border jumps, vital near fragile South Sudan.
For global readers, this reinforces avoiding high-risk travel to affected zones, monitoring post-exposure for 21 days, and supporting outbreak aid. Practical steps include handwashing, not touching bats/primates in endemic areas, and seeking care for fever after such exposure—reducing human-to-human chains breaks transmission.
Challenges, Limitations, and Outlook
Detection relies on alert systems, but rural access delays reporting; concurrent emergencies dilute focus. No therapeutics mean reliance on supportive care, where infrastructure gaps elevate fatality. Counterarguments note lower-end CFRs (24%) with optimal intervention, urging investment in vaccines nearing efficacy data.
Limitations include evolving case counts and untested probables; genetic analysis links it to East African strains, per EPHI. Sustained engagement remains pivotal—religious leaders’ role exemplifies culturally attuned strategies. As of November 29, no new deaths reported, but monitoring persists.
Medical Disclaimer: This article is for informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making any health-related decisions or changes to your treatment plan. The information presented here is based on current research and expert opinions, which may evolve as new evidence emerges.
References
-
World Health Organization. “Marburg virus disease – Ethiopia.” Disease Outbreak News, November 20, 2025. https://www.who.int/emergencies/disease-outbreak-news/item/2025-DON585who
-
Centers for Disease Control and Prevention. “Marburg Outbreak in Ethiopia: Current Situation.” November 25, 2025. https://www.cdc.gov/marburg/situation-summary/index.htmlcdc
-
Outbreak News Today. “Ethiopia Marburg death toll rises to 8.” Substack, November 27, 2025. https://outbreaknewstoday.substack.com/p/ethiopia-marburg-death-toll-rises









{kind=link}