
On 20 September 2022, Uganda health authorities declared an outbreak of Ebola disease, caused by Sudan virus, following laboratory confirmation of a patient from a village in Madudu sub-county, Mubende district, central Uganda.
As of 25 September 2022, a cumulative number of 18 confirmed and 18 probable cases have been reported from Mubende, Kyegegwa and Kassanda districts, including 23 deaths, of which five were among confirmed cases (CFR among confirmed cases 28%). This is the first Ebola disease outbreak caused by Sudan virus (SUDV) in Uganda since 2012.
Description of the outbreak
On 20 September 2022, the health authorities in Uganda declared an outbreak of Ebola disease caused by Sudan virus (SUDV), after a case was confirmed in a village of Madudu sub-county in Mubende district, central Uganda.
The case was a 24-year-old male who developed a wide range of symptoms on 11 September including high-grade fever, tonic convulsions, blood-stained vomit and diarrhoea, loss of appetite, pain while swallowing, chest pain, dry cough and bleeding in the eyes. He visited two private clinics, successively between 11-13 and 13-15 September without improvement. He was then referred to the Regional Referral Hospital (RRH) on 15 September where he was isolated as a suspected case of viral haemorrhagic fever. A blood sample was collected on 17 September and sent to the Uganda Virus Research Institute (UVRI) in Kampala where RT- PCR tests conducted were positive for SUDV on 19 September. On the same day, the patient died.
Results of preliminary investigations identified a number of community deaths from an unknown illness in Madudu and Kiruma sub-counties of Mubende district reported in the first two weeks of September. These deaths are now considered to be probable cases of Ebola caused by SUDV.
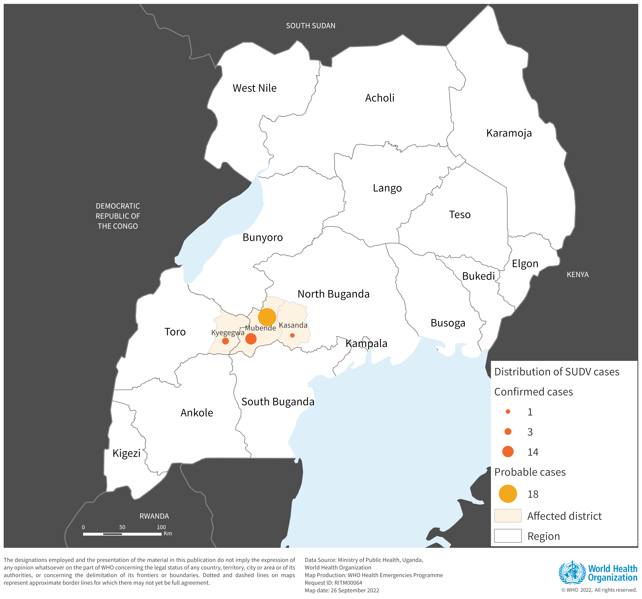
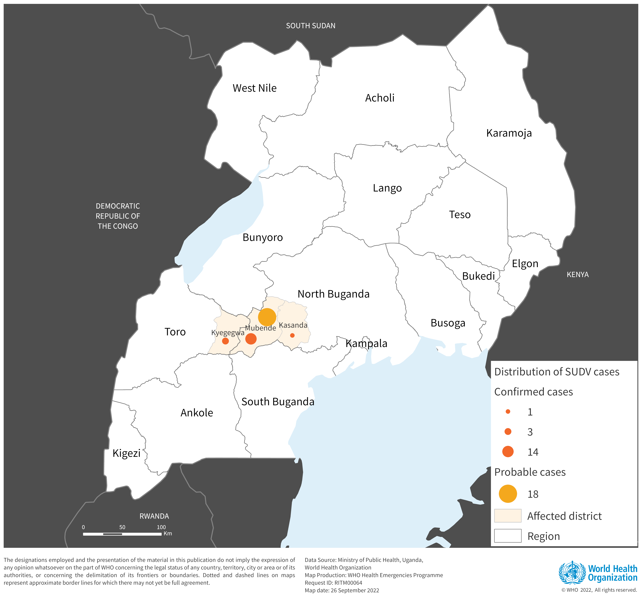
As of 25 September 2022, a cumulative number of 36 cases (18 confirmed and 18 probable cases) have been reported from Mubende (14 confirmed and 18 probable), Kyegegwa (three confirmed cases) and Kassanda (one confirmed case) districts. Twenty-three deaths have been recorded, of which five were among confirmed cases (CFR among confirmed cases 28%). Of the total confirmed and suspected cases, 62% are female and 38% are male. There are currently 13 confirmed cases hospitalized. The median age of the cases is 26 years (range 1 year to 60 years). A cumulative number of 223 contacts have been listed.
Map of confirmed (n=18) and suspected (n=18) cases of Ebola disease caused by Sudan virus, by district, Uganda (as of 25 September 2022).
Epidemiology of the disease
According to the International Classification of Disease for filoviruses (ICD-11) released in May 2019, Ebola disease is now sub-categorized depending on the causative virus. Outbreaks of Ebola disease caused by Sudan virus are named Sudan Virus Disease (SVD) outbreaks. Prior to May 2019 all viruses causing Ebola disease were grouped together. Based on the results of laboratory tests, this outbreak is caused by Sudan virus.
Sudan virus disease is a severe, often fatal illness affecting humans. Sudan virus was first reported in southern Sudan in June 1976, since then the virus has emerged periodically and up to now, seven outbreaks caused by SUDV have been reported, four in Uganda and three in Sudan. The estimated case fatality ratios of SVD have varied from 41% to 100% in past outbreaks.
The virus is introduced into the human population through close contact with the blood, secretions, organs or other bodily fluids of infected animals such as fruit bats, chimpanzees, gorillas, monkeys, forest antelope or porcupines found ill or dead or in the rainforest. The virus then spreads through human-to-human transmission via direct contact (through broken skin or mucous membranes) with either blood or body fluids of a person who is sick with or has died from SVD or objects that have been contaminated with body fluids (like blood, faeces, vomit) from a person sick with SVD or the body of a person who died from SVD.
The incubation period ranges from 2 to 21 days. People infected with Sudan virus cannot spread the disease until they develop symptoms, and they remain infectious as long as their blood contains the virus. Symptoms of SVD can be sudden and include fever, fatigue, muscle pain, headache, and sore throat later followed by vomiting, diarrhoea, rash, symptoms of impaired kidney and liver function. In some cases, the patient might present both internal and external bleeding (for example, bleeding from the gums, or blood in the stools).
The diagnosis of SVD can be difficult, as early nonspecific manifestation of the disease may mimic other infectious diseases such as malaria, typhoid fever and meningitis. Confirmation is made using numerous diagnostic methods including RT-PCR. Supportive care – rehydration with oral or intravenous fluids – and treatment of specific symptoms improve survival.
There are no licensed vaccines or therapeutics for the prevention and treatment of Sudan virus disease.
Uganda has reported four SVD outbreaks, in 2000, 2011 and 2012 (two outbreaks). Uganda also reported a Bundibugyo virus disease outbreak in 2007 and an Ebola virus disease outbreak in 2019.
Public health response
Coordination
- The Ministry of Health (MOH) established a National Task Force, with WHO providing technical support
- The Incidence Management Team was activated both within the MOH and the WHO country office
- The MOH Incident Commander has been deployed to Mubende District to support response efforts in the affected region
- WHO is supporting the orientation of the leadership at the Regional Referral Hospital and the district health team on early identification and case management
- A response plan is being developed and priority actions have been identified
Surveillance and Laboratory
- WHO has supported the activation of surveillance structures in districts
- Contact tracing and active case finding are ongoing
- WHO has deployed a technical team in Mubende district to support surveillance
Case Management
- WHO has supported the assessment of the isolation unit at the regional referral Hospital and dispatched an Ebola disease kit and tent for the isolation of patients
- WHO has deployed a central team of experts to support the establishment of a treatment unit in the Regional Referral Hospital
- Infection prevention and control (IPC) teams were deployed to support capacity building of health workers in IPC and the establishment of screening and triage at all health facilities in affected districts
Communication and Risk Communication
- As part of the communication and risk communication activities, WHO provided technical support for the organization of the press conference on Ebola and the development and dissemination of a press statement by the Ministry of Health
- Currently, WHO is supporting the review of Information, Education and Communication (IEC) material for dissemination to the public
WHO risk assessment
Uganda has experience in responding to Ebola virus disease and Sudan virus disease outbreaks, and necessary action has been initiated quickly. The current outbreak is the first Ebola disease outbreak caused by Sudan virus in Uganda since 2012.
In the absence of licensed vaccines and therapeutics for prevention and treatment of Sudan virus disease, the risk of potential serious public health impact is high. Community deaths and care of patients in private facilities and hospitals and other community health services with limited protection and infection prevention and control measures entail a high risk of many transmission chains. Investigations are ongoing to determine the scope of the outbreak and the possibility of spreading to other districts. Importation of cases to neighbouring countries cannot be ruled out at this stage.
According to the information currently available, the overall risk has been assessed as high at national level considering: (i) the confirmed Sudan virus and the lack of an authorized vaccine (ii) the possibility that the event started three weeks before the identification of the index case and several transmission chains have not been not tracked; (iii) patients presented at various facilities with suboptimal infection, prevention and control (IPC) practices including inadequate use of personal protective equipment (PPE); the patients died and were traditionally buried with large gathering ceremonies; (iv) although the country has developed an increased capacity to respond to Ebola outbreaks over recent years, and has a local capacity that can be easily mobilized and organised with available resources to mount a robust response, the system could be overwhelmed if the number of cases increases and the outbreak spreads to other sub-counties, districts and regions, as the country simultaneously responds to multiple emergencies, including anthrax, COVID-19, Rift Valley fever and Yellow fever, as well as flooding and prevailing food insecurity.
In addition, the outbreak was detected among individuals living around an active local gold mine. Mobility among traders of this commodity is likely to be high, and the declaration of the outbreak may cause some miners already incubating the disease to flee.
The currently affected Mubende district has no international borders. Nevertheless, the risk of international spread cannot be ruled out due to the active cross-border population movement. In addition, investigations are ongoing to establish transmission chains and the scope of the outbreak is yet to be determined.
At Regional and Global levels, the overall risk has been assessed as low.
WHO advice
Effective outbreak control relies on applying a package of interventions, including case management, surveillance and contact tracing, an optimal laboratory service, implementation of infection prevention and control measures in health care and community settings, safe and dignified burials and community engagement and social mobilization. Community engagement is essential to successfully controlling outbreaks. Raising awareness of risk factors for Ebola infection and protective measures that individuals can take is an effective way to reduce human transmission.
Early initiation of supportive treatment has been shown to significantly reduce deaths from Ebola disease. There is a need to strengthen surveillance and other response activities to contain the possibility of exponential spread.
Based on available evidence the ERVEBO vaccine — used in the recent responses against the Ebola virus disease outbreaks — will not provide cross-protection against the Sudan virus disease.
The Johnson & Johnson (Janssen) vaccine called Zabdeno/Mvabea against Ebola has only been approved by the European Medicines Agency (EMA) against Ebola virus disease and has not been tested against Sudan virus disease. This vaccine is administered on a two-dose schedule and requires 56 days between the two doses. The first dose provides protection against the Zaire ebolavirus and the second dose was designed to provide protection against other species of the virus, including Sudan. However, this multiantigen protection has not been demonstrated with clinical data. Even if the vaccine was tested and proved to be effective against Sudan ebolavirus, it would only provide protection some days after the second dose is administered. This means the vaccine is not appropriate for outbreak response.
WHO advises against any restrictions on travel and/or trade to Uganda based on available information for the current outbreak.
Further information
- Uganda declares Ebola Virus Disease outbreak, WHO AFRO: https://www.afro.who.int/countries/uganda/news/uganda-declares-ebola-virus-disease-outbreak
- Ebola virus disease fact sheet: http://www.who.int/en/news-room/fact-sheets/detail/ebola-virus-disease
- Optimized Supportive Care for Ebola Virus Disease. Clinical management standard operating procedures. WHO. 2019.
- Safety of two Ebola virus vaccines
- Personal protective equipment for use in a filovirus disease outbreak: rapid advice guideline
- Framework and toolkit for infection prevention and control in outbreak preparedness, readiness and response at the national level
- ICD-11 2022 release
- New filovirus disease classification and nomenclature
- Ministry of Health – Uganda, Official Twitter Account (Ebola outbreak situation update -25 September 2022)
Citable reference: World Health Organization (26 September 2022). Disease Outbreak News; Ebola Disease caused by Sudan virus – Uganda. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON410









{kind=link}