

Description of the outbreak
From when the outbreak was declared on 20 September until 7 November, a total of 136 confirmed cases and 53 confirmed deaths (CFR 38.9%) from Ebola disease caused by the Sudan ebolavirus (SUDV) have been reported, representing an increase of 18% and 66% respectively since the last DON published on 28 October 2022. In addition, 21 probable deaths have been also reported since the beginning of the outbreak, with the last probable death notified on 29 September. Three additional cases and three additional deaths have been reported among healthcare workers since 28 October, resulting in a total of 18 cases and seven deaths among these workers.
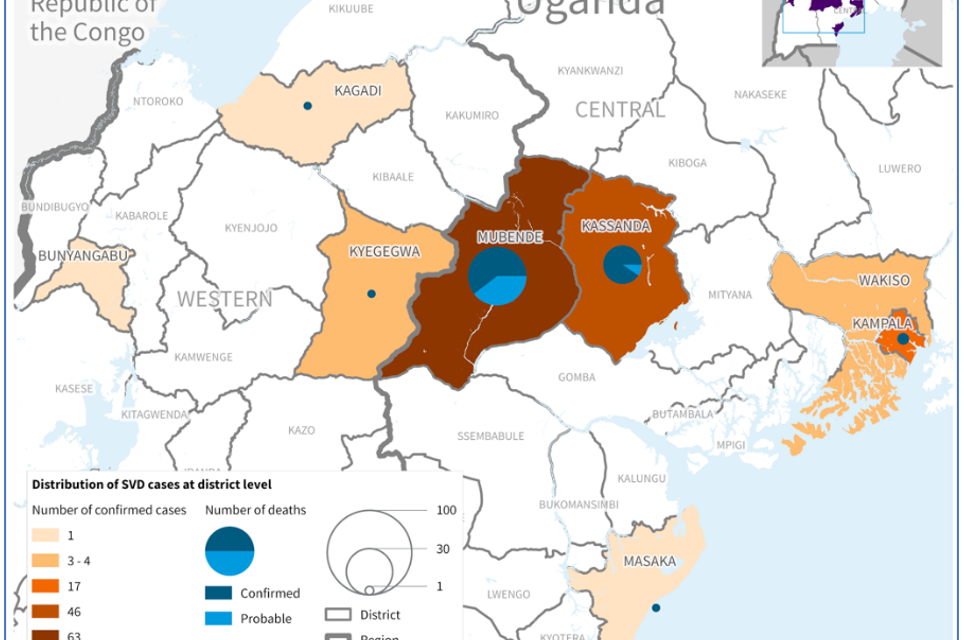
Since the last DON, one newly affected district has been reported (Masaka), leading to a total of eight districts reporting cases. The most affected district remains Mubende with 63 (46%) confirmed cases and 29 (55%) confirmed deaths, followed by Kassanda with 46 (34%) confirmed cases and 19 (36%) confirmed deaths. Two districts, Bunyangabu and Kagadi, have not reported cases for more than 40 days.
As of 7 November, a total of 1386 contacts in seven districts are currently under surveillance, with a follow-up rate of 92%. In the week commencing 31 October, an average of 1586 contacts were followed up daily, a decrease of 16% from the previous week (week commencing 24 October) when a daily average of 1896 contacts were followed up. A total of 34 contacts developed symptoms during the past week. Since the beginning of the outbreak, 3867 contacts have been registered, of which 2237 (68%) have completed the 21-day follow-up period.
As of 7 November, at least 2835 alerts have been received at a daily average of 71 alerts. Approximately 94% (n=2671) of all alerts received were investigated within 24 hours, of which 1120 were validated as suspected cases. The proportion of alerts investigated within 24 hours has been steadily increasing, and in the week commencing 31 October, nearly all alerts (657/659) were investigated within 24 hours, of which 31% (n=203) were validated as suspected cases.
Since the beginning of the outbreak, a total of 2139 samples were collected (suspects, repeat samples, swabs), of which 419 in the week commencing on 31 October (+11% increase as compared to the previous week when 377 samples were collected and tested).
Figure 1. Cases (confirmed and probable) and deaths (confirmed) of Ebola disease caused by SUDV by date of illness onset, as of 7 November 2022. 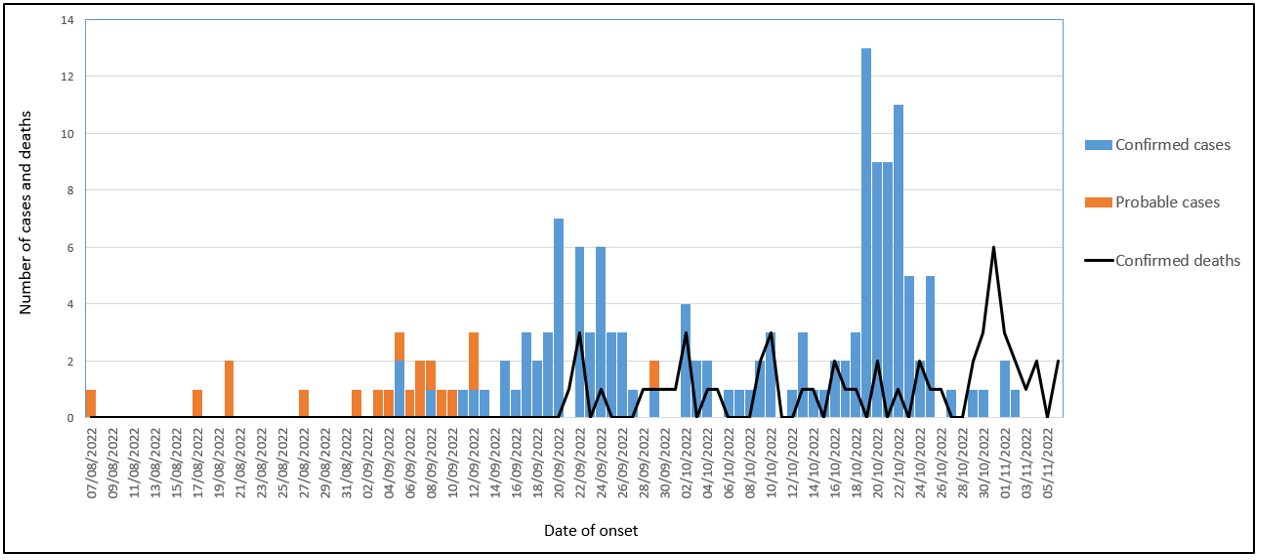 Graph re-produced using data reported in the Ministry of Health Uganda and WHO Situation Reports
Graph re-produced using data reported in the Ministry of Health Uganda and WHO Situation Reports
Table 1. Number of Cases (confirmed and probable) and deaths (confirmed) of Ebola disease caused by SUDV, by district, as of 7 November. 
Figure 2. Map of confirmed cases and deaths of Ebola disease caused by SUDV, by district, as of 7 November 2022. 
Public health response
For further information on the public health response in Uganda by the Ministry of Health, WHO and partners, see the latest situation reports jointly published by the Ministry of Health and the WHO Regional Office for Africa: https://www.afro.who.int/countries/publications?country=879.
Partners in the Global Outbreak Alert and Response Network (GOARN) have deployed staff to support the response activities in Uganda, primarily for case management, infection prevention and control and WASH, epidemiology and surveillance, laboratory, Risk Communication and Community Engagement (RCCE) and Safe and. Dignified Burials (SDBs).
Preparedness and operational readiness in neighboring countries
The Ministry of Health in the six neighboring countries (Burundi, the Democratic Republic of the Congo, Kenya, Rwanda, South Sudan, and the United Republic of Tanzania), in-country and international partners, and WHO are supporting SUDV readiness actions. These include the activation of multi-sectoral coordination mechanisms for SUDV; refresher training of rapid response teams; refresher laboratory training; infection prevention and control at health care facilities; activation/strengthening of surveillance systems for SUDV; community engagement and risk communication; screenings at points of entry (PoE) and assessment and reinforcement of case management capacities, among other activities.
Countries are requested to cascade the operational readiness activities to sub-national levels in high-risk districts/states to stop the introduction of SUDV into their communities. A new online preparedness assessment tool has been developed to measure key performance indicators to quantify and document the functionality of preparedness capacities in multiple high-risk districts in Uganda and six countries neighboring Uganda to facilitate real-time monitoring of the actual readiness status.
In addition, external stakeholders in these six countries will jointly assess preparedness. The Joint Assessment Missions (JAM) will evaluate preparedness at the national level as well as in high-risk subnational-level districts/states. The JAM reports will provide a detailed picture of preparedness capacities in all pillars and in all subnational areas that are at risk.
WHO risk assessment
On 1 November 2022, WHO revised the risk assessment for this event from high to very high at the national level, and from low to high at the regional level, while the risk remained low at the global level.
The estimated very high risk at the national level is based on a combination of several factors including the lack of licensed medical countermeasures; the late detection of the SUDV outbreak and its spread to multiple districts (including to larger cities like Kampala, with a population of more than four million people and travel connections to many neighbouring countries); a highly mobile population with reports of some high-risk contacts and symptomatic cases traveling between districts using public transportation; despite significant case-finding efforts, there is a possibility that some contacts may have been missed; reported challenges with community engagement in affected districts; many cases have presented at various health facilities with suboptimal infection prevention and control (IPC) practices.
The current outbreak is the first outbreak of Sudan ebolavirus in Uganda since 2012. Uganda has developed an increased capacity to respond to Ebola outbreaks over recent years and has a local capacity mobilized and organized with available resources to provide a robust response, but the system could be overwhelmed if the number of cases continues to rise and the outbreak spreads to other densely populated districts, as the country is simultaneously responding to multiple emergencies including outbreaks of anthrax, COVID-19, Crimean-Congo Haemorrhagic Fever, Rift Valley fever and yellow fever, as well as prevailing food insecurity.
At the regional level, the risk has been assessed as high due to the lack of licensed vaccines and therapeutics, mass population movements within and across neighbouring countries, along with weak cross-border surveillance that further amplifies the risk of disease spread, and health systems that respond to multiple emergencies.
The risk will be continuously assessed based on available and shared information.
WHO advice
Successful SUDV outbreak control relies on applying a package of interventions, including clinical management, community engagement, surveillance and contact tracing, and strengthening laboratory capacity.
Implementation of IPC measures in health care (e.g., hand hygiene, training of health workers, adequate personal protective equipment (PPE) supplies, waste management, environmental cleaning, and disinfection etc.) with ongoing monitoring and supervision for implementation is required to reduce risks of health care facilities amplifying the outbreak. Ensuring the provision of safe and dignified burials, supporting IPC in community settings (including adequate WASH facilities, hand hygiene capacity and safe waste management) and community engagement and social mobilization are essential to prevent and mitigate ongoing transmission.
Upon case identification, early initiation of supportive treatment has been shown to significantly reduce deaths from SUDV.
Establishing active surveillance at points of entry is an essential component of the outbreak response to mitigate the risk of international spread due to the high cross-border mobility between Uganda and neighbouring countries.
WHO advises against any restrictions on travel and/or trade to Uganda based on available information for the current outbreak.
Further information
- WHO AFRO: Uganda declares Ebola Virus Disease outbreak
- WHO AFRO. Ebola Virus Disease in Uganda SitReps
- WHO AFRO. Outbreaks and Emergencies Bulletin, Week 44: 24-30 October 2022
- WHO. Ebola, Uganda, 2022
- WHO Emergency Appeal: Ebola Disease Outbreak in Uganda
- Ministry of Health of the Republic of Uganda
- World Health Organization (26 September 2022). Disease Outbreak News; Ebola Disease caused by Sudan virus – Uganda. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON410
- World Health Organization (28 October 2022). Disease Outbreak News; Ebola disease caused by Sudan Ebola virus – Uganda. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON421
- Ebola virus disease fact sheet
- Optimized Supportive Care for Ebola Virus Disease. Clinical management standard operating procedures. WHO. 2019.
- Personal protective equipment for use in a filovirus disease outbreak: rapid advice guideline
- World Health Organization. (2021). Framework and toolkit for infection prevention and control in outbreak preparedness, readiness and response at the national level. World Health Organization. https://apps.who.int/iris/handle/10665/345251. License: CC BY-NC-SA 3.0 IGO
- Global health agencies outline plan to support Ugandan government-led response to outbreak of ebola virus disease
- ICD-11 2022 release
- Kuhn JH, Adachi T, Adhikari NKJ, et al. New filovirus disease classification and nomenclature. Nat Rev Microbiol. 2019;17(5):261-263. doi:10.1038/s41579-019-0187-4
Citable reference: World Health Organization (10 November 2022). Disease Outbreak News; Ebola disease caused by Sudan ebolavirus – Uganda. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON423










{kind=link}