
Measles is endemic in Afghanistan, with almost all provinces reporting suspected cases every year. Following periods of lower transmission in 2019 and 2020, and amid the humanitarian crisis in Afghanistan, weekly notifications of suspected measles cases have been increasing in all provinces since the end of July 2021, with the highest weekly toll observed in the last four weeks in January 2022 (Figure 1). The number of cases and deaths increased by 18% and 40% respectively from week 4, 2022 (week commencing January 24) to week 5, 2022 (week commencing January 31).
Figure 1. Weekly number of reported suspected measles cases in Afghanistan. Week 1, 2018 to week 4, 2022. Source: WHO Country Office in Afghanistan, WHO Regional Office for the Eastern Mediterranean.

From 1 January 2021 to 29 January 2022, 35 319 suspected measles cases were reported in Afghanistan, of which 3221 (9%) were laboratory-confirmed by IgM-ELISA in the seven reference laboratories (one national and six regional). Most of the suspected measles cases (91%) occurred among children less than 5 years of age. During the same period, 156 measles deaths were reported among the confirmed cases (CFR=4.8%), with more than 97% of the fatalities registered among children less than 5 years of age. Although the number of deaths is relatively low, the rapid rise in cases suggests that the trend of reported deaths will continue to increase sharply in the coming weeks.
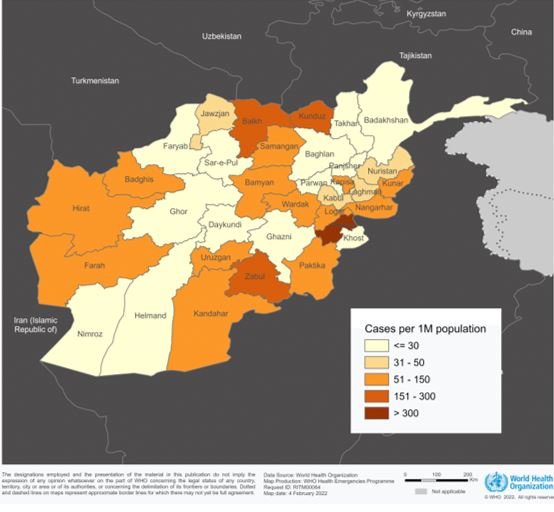
The most affected provinces, with the highest number of reported cases (confirmed and suspected) are Balkh, Ghazni, Helmand, Kandahar, Kabul, Paktika, and Paktya. Figure 2 shows the measles notification rate (confirmed and suspected cases) per million population. The highest rates were observed in Paktya (617 cases per 1 000 000), Balkh (275 cases per 1 000 000), Kunduz (204 cases per 1 000 000) Zabul (168 cases per 1 000 000), Kandahar (145 cases per 1 000 000), Logar (127 cases per 1 000 000).
Figure 2. Number of reported measles cases (confirmed and suspected) per million population by province, Afghanistan, January 2021 – January 2022. Source: WHO Country Office in Afghanistan, WHO Regional Office for the Eastern Mediterranean.

Public health response
- In December 2021, a measles outbreak response immunization campaign reached 1 510 440 children aged 9 to 59 months in Balk, Ghazni, Ghor, Helmand, Kandahar, and Paktika provinces. The campaign was implemented at fixed sites like mosques, schools and other suitable places easily accessible for parents. The highest administrative immunization coverage was reported in Ghor province (121%) and the lowest was reported in Ghazni province (90%). The next nationwide measles immunization campaign will be conducted in the first quarter of 2022.
- In the provinces where campaigns were conducted, implementing partners are supporting case management, risk communication and community engagement in the affected villages and surrounding areas.
- Vitamin A supplementation was provided to all children aged 6 to 59 months in November 2021 during the nationwide Polio campaign.
- WHO is providing technical support on surveillance, vaccination, laboratory testing, case management, and risk communication and together with the Health Cluster, WHO is continuing to coordinate and support a multi-pronged health response.
- Since November 2021, with emergency funding, WHO is delivering essential life-saving maternal and child health services in 17 provinces through 1209 Sehatmandi health facilities.
- As part of an emergency response to treat more than 1000 hospitalized children suffering from severe acute malnutrition, WHO supports 123 health clinics specialized in the management of severe acute malnutrition and airlifted 34.6 tons of life-saving health supplies to Afghanistan. The supplies include enough medicines to treat 15 000 people in need of medical care for three months.
- WHO provided technical and financial support for the establishment of the regional reference laboratory in Paktya province and supported 1131 health facilities to provide essential health services from November 2021 to January 2022, including medical referral facilities.
WHO risk assessment
Measles is a very highly contagious, vaccine-preventable disease caused by a virus that is transmitted by air and through direct contact with infected cases. Unvaccinated young children are at the highest risk of measles and its complications (e.g. pneumonia and encephalitis), including death. Measles outbreaks can result in epidemics with a high case fatality rate, especially among young, malnourished children.
Afghanistan is considered a fragile, conflict-affected and vulnerable setting. The country has faced years of compounded crises, under-investment, instability and drought, and has now the highest number of people in emergency food insecurity in the world. According to UNICEF, 14 million people in Afghanistan are facing acute food insecurity, and an estimated 3.2 million children under five years suffer from acute malnutrition.
The large and widespread outbreaks and the increasing number of reported measles cases in Afghanistan is due to a variety of complex factors that on the one hand have resulted in the low immunization coverage of both first dose of measles-containing vaccine (MCV1) and second dose (MCV2), on the other has exacerbated the impact of the outbreak (e.g. high levels of acute malnutrition, winter conditions and crowded domestic situation, previous displacement). 2020 WHO/UNICEF national immunization coverage estimates were 66% for MCV1 and 43% for MCV2. At the sub-national level, administrative coverage data shows that six provinces achieved less than 50% MCV1 coverage (Kandahar 40%; Paktya 38%; Jozjan 37%; Khost 36%; Helmand 18%; Urozgan 3.1%). The internal displacement of 698 000 people in 2021 was another driver of low MCV coverage. Internally displaced persons (IDPs) frequently live in conditions that increase susceptibility to measles (e.g. through less access to immunization services) and may increase measles exposures (e.g. through over-crowding) as well as experiencing poor health outcomes (e.g. due to factors like increasing risk and rates of malnutrition, poor access to curative services). Cross-border travel due to the recent instability in Afghanistan has increased the risk of international spread, particularly in Pakistan and Iran.
Overall risk at the national level is assessed as very high due to:
- Prolonged low measles vaccination coverage has led to the accumulation of a large susceptible population.
- High number of internally displaced people.
- High rates of malnutrition and vitamin A deficiency could result in increased mortality and are expected to increase especially in remote areas during the winter.
- Inadequate case management due to a shortage of equipment, supplies, and skilled staff in health facilities, long and difficult access to health facilities during the winter period.
- Barriers to access to healthcare in the rural population.
The regional risk is considered moderate due to the movement of people to Tajikistan, Iran and Pakistan, while at the global level the risk is considered low due to moderately high global MCV coverage estimates. More information is required from neighbouring countries and continued monitoring of displacement trends.
WHO advice
Two-dose measles vaccination coverage of at least 95% in every province is recommended to ensure immunity. Strengthening routine immunization and conducting outbreak response immunization campaigns are essential for effective control of the epidemic and reducing mortality.
The administration of vitamin A, particularly in the context of malnutrition, is critical to reducing morbidity and mortality. Other essential measles prevention and response interventions, include:
- Ensure a rapid, effective response to current measles outbreaks in Q1 2022. And ensure systems are established and strengthened for routine immunization and the planned SIA later in 2022.
- Ensure high-quality measles case-based surveillance as a critical strategy for outbreak control.
- Early detection and confirmation of measles cases to ensure timely and proper case management to reduce morbidity and mortality, enable implementation of appropriate public health strategies to control further transmission.
- Identify zero-dose populations and areas with low coverage and at higher risk of outbreaks that require enhanced vaccination efforts.
- Engage with communities to establish two-way dialogue by listening to community concerns and feedback and continually refining the outbreak response according to community needs and perspectives.
- Identify root causes of measles outbreaks so that immunity gaps and/or system weaknesses can be addressed to reduce the risk of future outbreaks.
- Strengthen vaccination of health workers to reduce transmission in health care settings and reduce the risk of spread to vulnerable populations.








{kind=link}