
Situation at a glance
Description of the situation
Angola reported its first cholera case in early January 2025. As of 23 March 2025, a cumulative total of 8543 cholera cases have been reported, including 329 deaths (CFR 3.9%), of which 112 (34%) occurred in the community. The CFR for hospitalised cases is 2.5%. Currently, 253 cases are hospitalized. The outbreak initially saw a rapid increase in cases, exceeding 1000 weekly cases in early February. This was followed by a decline and a plateau, with case numbers stabilizing at approximately 800 cases per week for a month. However, in the week of 23 March, cases surged again, reaching close to 1200 cases—the highest weekly count to date.
Figure 1. Number of cholera cases by epidemiological week of reporting (n=8543), as of 23 March 2025. Data source: República de Angola. Boletim de Cólera

The 6-14 year age group is the most affected, with 1976 cases, representing 23.1% of the total cases, followed by the 15-24 year age group with 1850 cases (21.7%), and the 25-34 year age group with 1475 cases (17.3%). Slightly over half of reported cases are male (4725; 55.3%).
Figure 2. Age-gender distribution of cholera cases (n=8543), as of 23 March 2025. Data source: República de Angola. Boletim de Cólera 
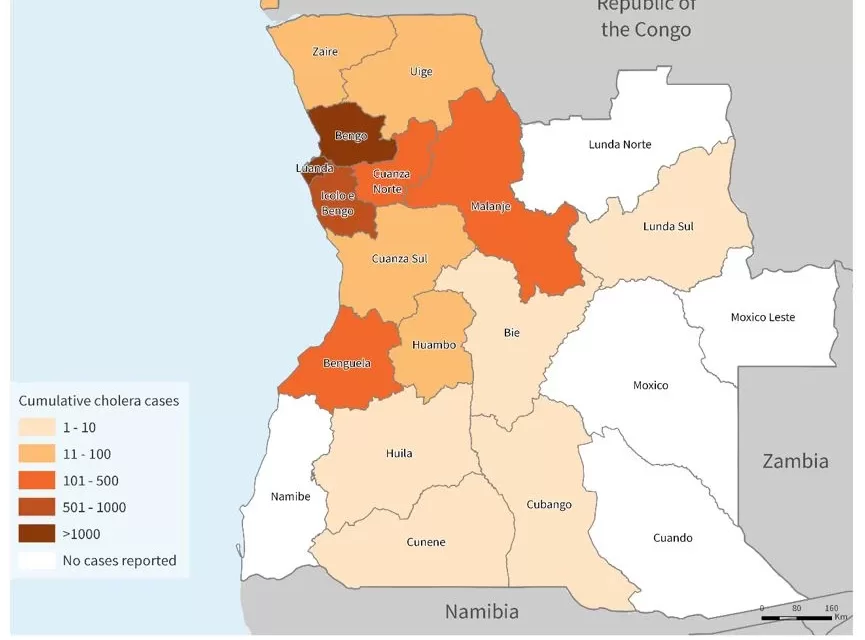
The cholera outbreak is affecting 16 (76.2%) of the 21 Angolan provinces, with the highest number of cases reported from Luanda (4143; 48.5%) and Bengo (2485; 29.1%) provinces.
Figure 3. Map of cholera cases by province (n=8543), as of 23 March 2025. Data source: República de Angola.Boletim de Cólera 
Epidemiology
Cholera is an acute diarrheal infection caused by consuming food or water contaminated with the bacterium Vibrio cholerae. It is primarily associated with poor sanitation and limited access to safe water. The disease can cause severe acute watery diarrhea, resulting in significant morbidity and mortality. The speed of spread depends on exposure levels, population vulnerability, and environmental conditions. Cholera affects both children and adults and can be fatal if left untreated.
The incubation period ranges from 12 hours to five days after consuming contaminated food or water. While most infected individuals remain asymptomatic, they can still shed the bacteria in feces for up to 10 days, potentially spreading the infection to others. Among symptomatic cases, most experience mild to moderate illness, while a smaller proportion develop severe diarrhea and vomiting, which can lead to life-threatening dehydration. However, cholera is highly treatable, with most cases successfully managed through prompt administration of Oral Rehydration Solution (ORS).
Humanitarian crises and natural disasters, such as floods, heighten the risk of cholera transmission by disrupting water and sanitation systems and forcing populations into overcrowded, unsanitary conditions. Controlling cholera outbreaks requires a multisectoral approach, combining surveillance, WASH (water, sanitation, and hygiene) interventions, social mobilization, adequate case management, and oral cholera vaccination.
Angola has faced recurrent cholera outbreaks since the 1970s, with major surges in 1987 (16 000 cases, 1460 deaths) and 2006 (over 67 000 cases, 2700 deaths). After annual outbreaks from 1987 to 1996, cholera re-emerged in 2006 following a decade-long absence. Since then, periodic outbreaks—often linked to cholera activity in the adjacent Democratic Republic of the Congo, and worsened by poor water and sanitation—have occurred, notably in 2011–2013 and 2016–2018, with peaks during the rainy season.
Since 2021, there has been an increase in cholera cases and their geographical spread globally. Between 1 January and 23 March 2025, a total of 93 172 cases and 1197 deaths were reported across 24 countries spanning three WHO regions, with the African Region recording the highest numbers (55 622 cases from 18 countries).
Public health response
Coordination
- The Ministry of Health, supported by international partners such as WHO, UNICEF, and others, is leading efforts to mitigate the impact of the cholera outbreak. The Ministry is actively coordinating with local and international partners to ensure an efficient response, while reinforcing the health system’s capacity to manage the outbreak.
Epidemiological Surveillance and Laboratory
- WHO has trained over 120 health workers in active case detection and reporting, rapid infection surveys, data processing, and community mobilization for preventive measures.
- In Bengo province, WHO is supporting the deployment of 13 rapid response teams, which are working daily within affected communities to identify and respond to new cases.
- The Ministry of Health, with WHO’s support, is enhancing the capacity of data management experts in Luanda to improve case mapping, strengthen surveillance, and enhance case detection and analysis at health units.
- WHO is further assisting the government by reinforcing response teams to ensure the timely identification of affected individuals, support community engagement efforts, manage infection control measures, and protect the population.
Case Management
- Cholera treatment centers (CTCs) in Bengo province are being expanded to accommodate the increasing number of cases and enhance healthcare capacity.
- WHO is supporting case management by providing technical support, including the dissemination of treatment protocols and clinical posters.
- WHO has facilitated comprehensive training and supervision of clinical staff working in the cholera treatment units (CTUs) and CTCs across affected provinces.
- WHO has assisted in establishing CTCs, CTUs, and oral rehydration points (ORPs), expanding access to life-saving treatment.
Infection Prevention and Control (IPC)/Water, Hygiene, and Sanitation (WASH)
- UNICEF is supporting WASH initiatives by distributing hygiene supplies to over 64 500 children in 63 schools, ensuring that the most vulnerable populations have access to essential resources.
- The installation of water tanks in affected communities is helping to improve access to safe drinking water, a critical factor in controlling cholera transmission.
- Long-term improvements to water, sanitation, and hygiene infrastructures are being prioritized to mitigate the spread of cholera and other waterborne diseases, and to ensure sustainable solutions that align with broader public health goals.
Risk Communication and Community Engagement
- Community mobilization efforts to promote safe behaviors and increase vaccine uptake are underway, with support from religious leaders, community influencers, and local organizations.
- The WHO, alongside local partners, is conducting awareness campaigns to educate the public about the importance of proper hand hygiene, the use of latrines, and food safety.
Vaccination
- The Ministry of Health, with support from WHO, UNICEF, the World Bank, and the International Committee of the Red Cross, carried out a five-day reactive vaccination campaign in January 2025. Over 900 000 people were vaccinated, with a 99.5% administrative coverage rate.
- WHO has provided logistical support and operational guidance for the vaccination campaign, ensuring the efficient distribution of vaccines and the establishment of vaccination centers in affected areas.
- 700 000 additional doses of oral cholera vaccines arrived in country mid-March for a second reactive campaign.
Preparedness and Readiness
- A readiness assessment will be conducted to identify preparedness and readiness gaps across all response pillars. The findings will inform the development of a comprehensive plan to strengthen systems in unaffected areas, with the ultimate aim of limiting the spread of the outbreak.
WHO risk assessment
Angola is experiencing a substantial cholera outbreak with a significant proportion of deaths occurring in the community, exacerbating cholera transmission by delaying case detection and response, hindering timely public health interventions, and increasing environmental contamination through unsafe burials. The high CFR of 3.9% highlights critical challenges, including late case presentation, gaps in surveillance and early response, inadequate healthcare capacity, and barriers to accessing life-saving treatment, particularly in underserved areas. Inadequate access to clean water and sanitation continues to leave Angola highly vulnerable to cholera outbreaks, especially in densely populated urban centers and remote rural communities. The rainy season (October-April), with its associated heavy rainfall and flooding, directly amplifies this risk by contaminating water sources and facilitating rapid cholera transmission. Flood-prone provinces like Bengo face a heightened risk of further spread as the season progresses.
Angola shares borders with the Democratic Republic of Congo and Zambia, both currently experiencing cholera outbreaks. Frequent population movement between Angola and surrounding countries heightens the risk of cross-border transmission, particularly in high-mobility areas like Luanda.
WHO advice
WHO emphasizes the importance of timely and proper case management, ensuring access to safe drinking water, and improving sanitation infrastructure. Effective infection prevention and control measures are critical to reducing transmission of cholera and other pathogens that can cause health care-associated infections in facilities caring for patients with cholera. WHO recommends risk communication and community engagement interventions to build trust and empower communities with evidence-based information, enabling them to make informed decisions to protect their health.
Promoting preventive hygiene practices and food safety in communities is one of the most effective strategies to control cholera. Public health risk communication is vital to ensure that communities understand the importance of hygiene, safe food practices, and the use of oral rehydration solutions (ORS). Rapid access to ORS is essential, especially in rural areas where larger health centers may not be easily accessible. Educating communities on how to prepare ORS at home, along with emphasizing the importance of staying hydrated while seeking medical care, can significantly reduce the risk of severe outcomes. With timely care, the case fatality rate can be kept below 1%.
OCV campaigns are an important tool for controlling cholera outbreaks. When used alongside improvements in water and sanitation, OCV can help prevent the spread of cholera, particularly in high-risk areas. Strong risk communication efforts are needed to manage vaccine demand, inform communities about vaccine schedules, and build trust regarding the vaccine’s safety and efficacy.
WHO recommends that countries strengthen surveillance, particularly at the community level, for early detection of suspected cases and to prevent the spread of cholera. Cooperation between neighboring countries is crucial to control outbreaks, especially in regions with high cross-border movement. Strengthening these efforts will enable affected countries to effectively control and prevent cholera outbreaks, improving public health outcomes.
Further information
-
- WHO Cholera factsheet
- GTFCC, Public health surveillance for cholera: Interim guidance
- ENDING CHOLERA, A GLOBAL ROADMAP TO 2030
- Multi-country outbreak of mpox, External situation report #49 – 28 March 2025
- República de Angola. Boletim de Cólera
- WHO. Strengthening active cholera case finding in Angola
- WHO. Angola Enhances Data Management to Combat Cholera Outbreak
- UNICEF. Angola situation reports.
- UNICEF. Epidemiological study of cholera hotspots in Angola | October 2018 | Prospective and Cooperation
- WHO. Water, sanitation and hygiene and infection prevention and control measures for infectious diarrhoea in health-care settings
Citable reference: World Health Organization (28 March 2025). Disease Outbreak News; Cholera in Angola. Available at: http://www.who.int/emergencies/disease-outbreak-news/item/2025-DON562










{kind=link}