
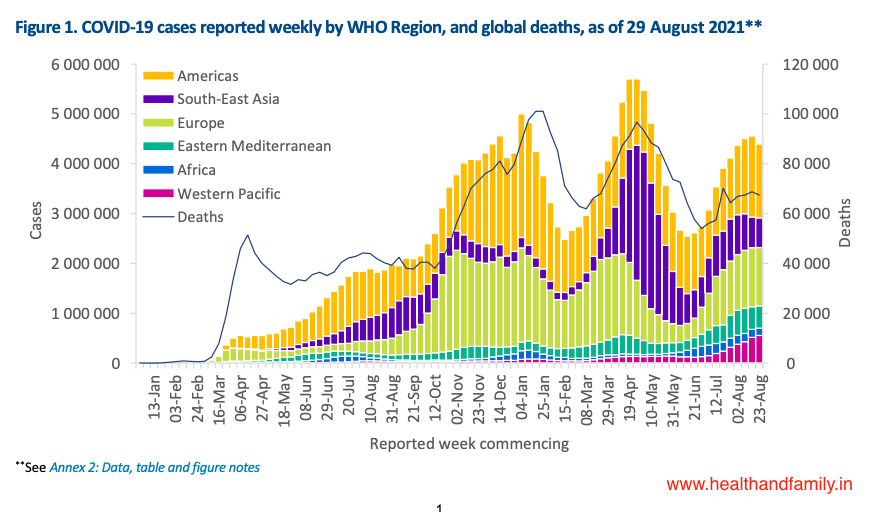
Global overview Data as of 29 August 2021
With just under 4.4 million new cases reported this week (23-29 August), the number of new cases reported globally remains similar to the previous week after having increased for nearly two months (Figure 1). In the past week, all regions reported either a decline (Regions of Africa and the Americas) or a similar trend (Europe, South-East Asia and Eastern Mediterranean Regions) in new cases, except for the Western Pacific Region which reported a 7% increase as compared to previous week.


The number of deaths reported globally this week was also similar to last week, with just over 67 000 new deaths reported. The Eastern Mediterranean and Western Pacific Regions reported an increase in the number of weekly deaths, 9% and 16% respectively, while the South-East Asia Region reported the largest decrease (20%). The numbers of deaths reported in the Regions of Africa, Europe and the Americas were similar to last week. The cumulative number of cases reported globally is now nearly 216 million and the cumulative number of deaths is just under 4.5 million.

The Regions reporting the highest weekly incidence rates per 100 000 population of cases and of deaths remain the same as last week: the Regions of the Americas (144.9 new cases per 100 000 population; 2.2 deaths per 100 000 population) and Europe (125.7 new cases per 100 000 population; 1.3 deaths per 100 000 population). The Eastern Mediterranean Region also reported a high incidence of weekly deaths (1.1 per 100 000 population).

The highest numbers of new cases were reported from the United States of America (938 014 new cases; 8% decrease), India (270 796 new cases; 17% increase), the Islamic Republic of Iran (254 753 new cases; similar to the previous week), the United Kingdom (237 556 new cases; 8% increase), and Brazil (175 807 new cases; 16% decrease).






Globally, cases of the Alpha variant have been reported in 193 countries (one new country since last week), territories or areas (hereafter countries), while 141 countries (no new countries) have reported cases of the Beta variant; 91 countries (five new countries) have reported cases of the Gamma variant; and 170 countries (seven new countries) have reported cases of the Delta variant.
Special Focus: Update on SARS-CoV-2 Variants of Interest and Variants of Concern
WHO, in collaboration with national authorities, institutions and researchers, routinely assesses if variants of SARS-CoV-2 alter transmission or disease characteristics, or impact vaccine, therapeutics, diagnostics or effectiveness of public health and social measures (PHSM) applied by national authorities to control disease spread.
As these risks evolve, WHO will continue to update lists of global VOIs and VOCs to support setting priorities for surveillance and research, and ultimately guide response strategies (for more information, please see the Tracking SARS-CoV-2 variants website).
National authorities may choose to designate other variants of local interest/concern and are encouraged to investigate and report on impacts of these variants.

As surveillance activities to detect SARS-CoV-2 variants are strengthened at national and subnational levels, including through the expansion of genomic sequencing capacities, the number of countries/areas/territories (hereafter countries) reporting VOCs continues to increase (Figure 4, Annex 1). This distribution should nonetheless be interpreted with due consideration of surveillance limitations, including differences in sequencing capacities and sampling strategies between countries.
As countries gradually resume non-essential international travel, the introduction of risk mitigation measures aiming to reduce travel-associated exportation, importation and onward transmission of SARS-CoV-2 should be based on thorough risk assessments conducted systematically and routinely.
Updates to the variant classifications
As the global public health risks posed by specific SARS-CoV-2 variants become better understood, WHO will continue to update the list of global VOIs and VOCs to support the setting of priorities for surveillance and research, and ultimately to guide response strategies. These updates reflect virus evolution and the emergence of new variants, changing epidemiology, as well as our evolving understanding of the phenotypic impacts of variants as new evidence becomes available. A previously designated Alert for further monitoring which subsequently meets the WHO working definition of a Variant of Interest (VOI) or Variant of Concern (VOC) can be reclassified.
Based on the latest round of assessments, B.1.621 was classified as a VOI on 30 August 2021 and given the WHO label “Mu”. This includes the descendent Pango lineage B.1.621.1. This variant is known as 21H in Nextstrain nomenclature. The Mu variant has a constellation of mutations that indicate potential properties of immune escape. Preliminary data presented to the Virus Evolution Working Group show a reduction in neutralization capacity of convalescent and vaccinee sera similar to that seen for the Beta variant, but this needs to be confirmed by further studies.
Since its first identification in Colombia in January 2021, there have been a few sporadic reports of cases of the Mu variant and some larger outbreaks have been reported from other countries in South America and in Europe. As of 29 August, over 4500 sequences (3794 sequences of B.1.621 and 856 sequences of B.1.621.1) have been uploaded to GISAID from 39 countries. Although the global prevalence of the Mu variant among sequenced cases has declined and is currently below 0.1%, the prevalence in Colombia (39%) and Ecuador (13%) has consistently increased. The reported prevalence should be interpreted with due consideration of sequencing capacities and timeliness of sharing of sequences, both of which vary between countries. More studies are required to understand the phenotypic and clinical characteristics of this variant. The epidemiology of the Mu variant in South America, particularly with the co-circulation of the Delta variant, will be monitored for changes.









{kind=link}