
In Pakistan, cholera is endemic with an epidemic threshold of a single laboratory confirmed case.
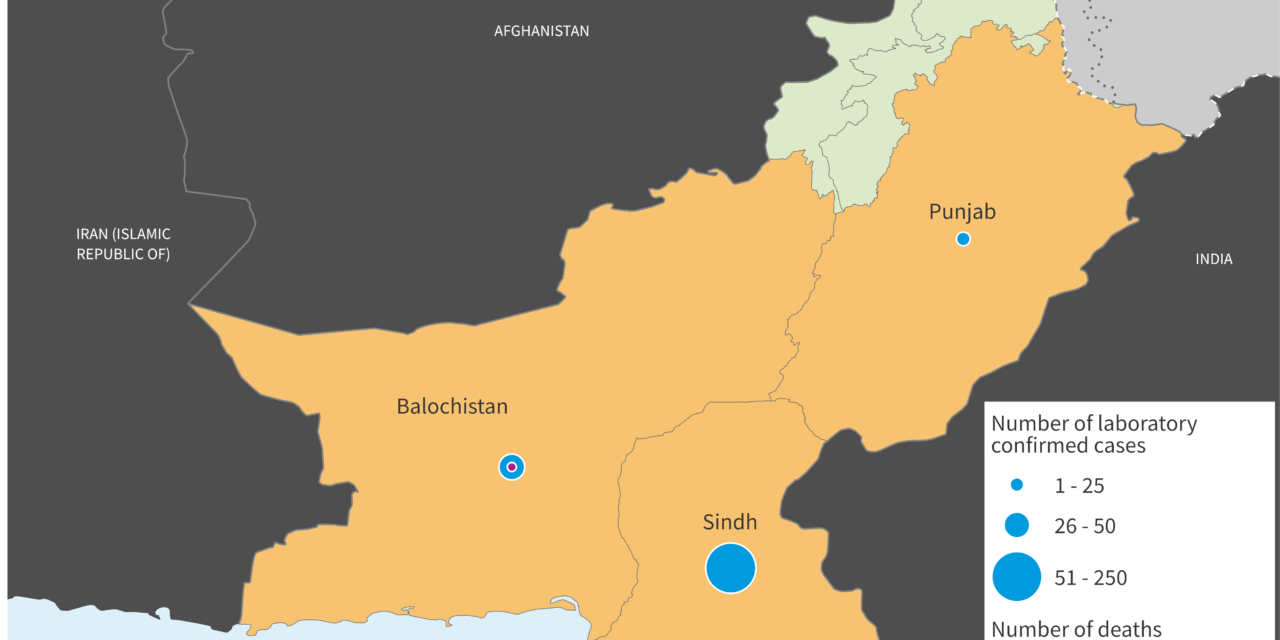
In 2022, Sindh province is facing a significant increase in cholera cases with 234 laboratory confirmed cases reported between 15 January to 27 May. Balochistan and Punjab provinces have also reported 31 and 25 confirmed cases of cholera, respectively.
Currently, there is no evidence of cross-border spread of the disease. The risk of potential international spread exists given that Pakistan has long land borders with significant cross border movement and multiple major urban hubs including Karachi city in Sindh province, with international transport hubs.
Description of the outbreak
On 26 April 2022, the National IHR Focal Point of Pakistan reported a laboratory confirmed outbreak of cholera in Sindh province, Pakistan. As of 27 May, three provinces – Sindh, Balochistan, and Punjab, have reported a total of 290 confirmed cases of cholera.
The first laboratory confirmed case was reported on 15 January 2022 in Sindh province. Between 15 January and 27 May, 234 laboratory confirmed cases, with no deaths, have been reported from the province. Of these cases, 126 (54%) were females, and 114 (49%) were in children younger than nine years old. According to the cholera surveillance national policy, samples from children are prioritized over adults for confirmatory culture testing which may explain the high proportion of confirmed cases among children.
As of 27 May, a total of 109 samples have been tested from the public water sources (hydrants) and individual households in Karachi city, Sindh province. Among these, results are available for 71 samples, of which 70% have shown presence of Vibrio cholerae while Escherichia Coli and coliform was detected in 55% and 90% of samples, respectively.
In addition to Sindh province, three districts in Balochistan have reported 31 confirmed cases and nine deaths while two districts in Punjab have reported 25 confirmed cases.
Figure 1: Distribution of cholera cases in Pakistan, 15 January to 27 May 2022 (n=290)

Epidemiology of cholera
Cholera is an acute enteric infection caused by ingesting the bacteria Vibrio cholerae present in contaminated water or food. It is mainly linked to insufficient access to safe drinking water and inadequate sanitation. It is an extremely virulent disease that can cause severe acute watery diarrhoea resulting in high morbidity and mortality, and can spread rapidly, depending on the frequency of exposure, the exposed population and the setting. Cholera affects both children and adults and can be fatal if untreated.
The incubation period is between 12 hours and five days after ingestion of contaminated food or water. Most people infected with V. cholerae do not develop any symptoms, although the bacteria are present in their faeces for 1-10 days after infection and are shed back into the environment, potentially infecting other people. Among people who develop symptoms, the majority have mild or moderate symptoms, while a minority develop acute watery diarrhoea with severe dehydration. Cholera is an easily treatable disease. Most people can be treated successfully through prompt administration of oral rehydration solution (ORS).
Cholera can be endemic or epidemic. A cholera-endemic area is an area where confirmed cholera cases were detected during the last three years with evidence of local transmission (cases are not imported from elsewhere). A cholera epidemic can occur in both endemic countries and in non-endemic countries. Uninfected dead bodies have never been reported as the source of epidemics.
The consequences of a humanitarian crisis – such as disruption of water and sanitation systems, or the displacement of populations to inadequate and overcrowded camps – can increase the risk of cholera transmission, should the bacteria be present or introduced.
A multisectoral approach including a combination of surveillance, water, sanitation and hygiene, social mobilization, treatment, and oral cholera vaccines is essential to control cholera outbreaks and to reduce deaths.
Public health response
In response to the outbreak, the provincial health authorities of Sindh, Balochistan and Punjab have issued high alert notifications to concerned District Health Offices. The three provincial departments have also officially declared an outbreak in the affected districts.
A cholera response plan has been prepared and response activities are being implemented in the affected districts of Sindh, Balochistan and Punjab. This includes establishing sentinel surveillance sites, activating rapid response teams for follow-up of cases and engaging private sector hospitals to enhance reporting. Material support has also been provided to ensure the availability of supplies including ORS, zinc, selected antibiotics and intra venous fluids for case management. Community engagement and health education messages have been developed and disseminated in high-risk communities. Oral cholera vaccine (OCV) campaigns are being planned for affected areas.
WHO has provided support to health authorities in Pakistan through:
- Advocacy and coordination through multiple high-level meetings. This includes advocating and guiding appropriate authorities on the response to the cholera outbreak and providing support to the provincial cholera control cell.
- Technical support for surveillance, case management including infection, prevention and control (IPC), data management and social mobilization.
- Community engagement including support for social mobilizers in highly affected districts and health awareness sessions that are being conducted on a daily basis.
- Collaboration with partners such as UNICEF at the national and provincial level for implementation of effective water, sanitation and hygiene (WASH) interventions.
- Conducting field visits to various hospitals to support surveillance, laboratory testing for cholera confirmation, water quality monitoring, improving IPC measures and case management.
- Support to the affected districts through the distribution of sample collection kits, water purification tablets, ORS as well as information on cholera, education, and communication materials.
- Laboratory support to civil hospitals to conduct water and environmental sampling.
- Capacity building for district health management teams, health care providers and hospital focal persons on surveillance, rapid response teams and in areas including laboratory testing, IPC, and case management.
- Distribution of risk communication pamphlets and awareness banners with additional materials being printed for future distribution. Development of customized standard operation procedures for disease transmitted by the fecal-oral route and distribution to health care facilities to improve cholera case management.
- Submitted requests for OCV which were accepted by International Coordinating Group (ICG) for reactive campaigns in multiple affected areas.
WHO risk assessment
The risk of potential international spread from Sindh province exists given that the most affected districts are located in Karachi city which is an industrial center as well as transport hub with airport and seaport; it is also the largest city in Pakistan and capital of Sindh province. Currently, no international cross-border spread has been confirmed for this event. However, with ongoing transmission in close proximity to border areas and transportation hubs, the risk of international spread cannot be ruled out.
In Balochistan province, there is suboptimal surveillance, limited access to safe drinking water, and limited access to health care, and affected areas are in proximity to areas with active cross-border movement with Afghanistan and Iran.
In Punjab, although response activities are taking place, the province is still recording an increased number of suspected cholera cases, including in Lahore, the provincial capital and large international commercial hub. Further spread to other provinces would worsen the situation given the frequent population movement.
Necessary control measures are being implemented by the national authorities with support from WHO and partners to contain the outbreak, as described in the Public Health Response section above. However, there is a need to further strengthen surveillance by establishing systematic detection and laboratory confirmation of cholera to properly track the evolution of the outbreak and institute timely and appropriate interventions.
WHO advice
- WHO recommends strengthening of the disease surveillance system. Surveillance for early case detection, confirmation and response in other provinces and regions of Pakistan should be reinforced.
- Proper and timely case management of cholera cases should be ensured.
- Oral cholera vaccines should be used in conjunction with improvements in WASH activities to control cholera outbreaks and for prevention in areas known to be at high risk for cholera.
- Improving access to safe drinking water and sanitation infrastructure, as well as improving IPC measures in healthcare facilities, with hygiene practices and food safety in affected communities are the most effective means of controlling cholera.
- Risk communication and community engagement on cholera prevention and early care seeking and treatment should be provided to the population.
WHO does not recommend any travel or trade restrictions on Pakistan based on the currently available information.









{kind=link}