
Description of the Situation
On 1 November 2023, the IHR National Focal Point of Zambia notified WHO of an anthrax outbreak in humans. The first human cases were reported from the Dengeza Health Post in the Sinazongwe District of the Southern Province on 5 May 2023. Around the same period, domestic (cattle and goats) and wild animals (hippopotami) were reportedly dying from an unknown cause in the surrounding areas. While Zambia typically reports sporadic cases of anthrax annually, the investigation revealed that from September 2022 to January 2023, 42 suspected cases of anthrax in humans had been recorded at the Dengeza Health Post. All the cases presented at health facilities with skin sores and ulcers, and some of them developed nonspecific symptoms (e.g., nausea, vomiting, difficulty in breathing). Human specimens were collected during the investigation and sent to the Lusaka Central Veterinary Research Institute (CVRI) for testing. The initial samples collected and tested by culture returned negative for anthrax.
In June 2023, human and animal cases were reported in the Kanchindu and Siameja veterinary camps of Sinazongwe district. Twenty-six human cases developed sores on their face, arms, and fingers after consuming meat from three wild hippopotamus carcasses. The first human case was reported on 16 June 2023 and laboratory confirmed by culture at the Lusaka CVRI. On the animal side, 13 domestic animals including cattle (10) and goats (3) out of Sinazongwe district susceptible population of 65 000 (30 000 cattle and 35 000 goats), under free range extensive traditional management, died of suspected anthrax. Cattle and goat specimens tested by culture at the Lusaka CVRI returned positive for anthrax on 17 July 2023. Until 1 November, anthrax outbreaks affecting animals and humans were reported in other Southern, Northwestern, and Western provinces.
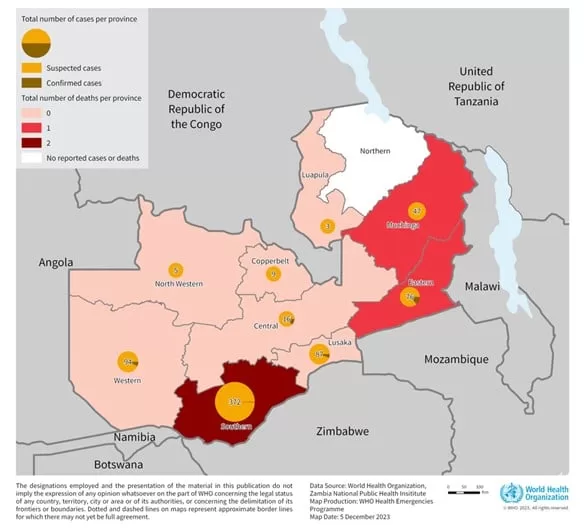
As of 20 November 2023, 684 suspected human cases, including four deaths (CFR 0.6%) were reported from 44 out of 116 districts in nine of Zambia’s 10 provinces. Sinazongwe district is the epicenter, accounting for 287 cases (42% of total 684 cases) and two deaths (50% of total the four deaths). The most affected provinces are the Southern (370 cases; 54 %), Western (84; 12%), Lusaka (82; 12%), Eastern (66; 10%) and Muchinga (47; 7 %) Provinces. The majority of symptomatic cases were epidemiologically linked to confirmed cases and not tested.
On the animal side, as of 21 November 2023, 568 domestic and wild animal cases were reported across 11 districts in Eastern, Southern, and Western provinces, with (344; 61%) occurring in the Southern province, (132; 23%) in the Muchinga province and (62, 11%) in the Western Province. Cases in wildlife, primarily hippos, were reported in the Eastern and Southern provinces.
This outbreak marks the first major occurrence spanning nine out of 10 country provinces. Previous outbreaks were confined to Northwest and Western provinces, with sporadic cases over the years. Of note, Zambia reported anthrax outbreaks in both human and animals in Western Province in 2017 and in Eastern Province in 2016 and 2011.
Figure 1. Distribution of anthrax cases by province, Zambia, as of 20 November 2023
Epidemiology
Anthrax is a disease caused by a spore-forming bacteria called Bacillus anthracis. It is a zoonosis (disease transmissible from animals to humans) that affects ruminants (such as cows, sheep, and goats). Anthrax does not typically spread from animal to animal or human to human. When anthrax spores are ingested from contaminated animal products, inhaled, or enter the body through skin abrasions or cuts, they can germinate, multiply and produce toxins.
Depending on the type of exposure, within a few hours to three weeks, individuals may present one of the three clinical presentations of anthrax.
- Cutaneous or skin anthrax is the most common presenting with an itchy bump in the exposed area that rapidly develops into a black sore. Some people then develop headaches, muscle aches, fever, and vomiting.
- Gastrointestinal anthrax causes initial symptoms similar to food poisoning, but can worsen to produce severe abdominal pain, vomiting of blood and severe diarrhoea.
Pulmonary anthrax, the most severe presentation, has initial symptomatology of a common cold but can rapidly progress to severe breathing difficulties and shock. Diagnosis can be made through polychrome methylene blue-stained blood smears, polymerase chain reaction (PCR) or enzyme-linked immunosorbent assay (ELISA). Hospitalization is required for all human cases identified. Individuals exposed may receive prophylactic treatment. Antibiotics, particularly penicillin, are effective against this disease. Prompt treatment can reduce case-fatality rate to <1%. Vaccines are also available for livestock and humans in limited supply. Human vaccines are limited to those with possible occupational exposure.
Public Health Response
Response activities have been taken from both human and animal sides.
Actions taken for animals
With the support of the Food and Agriculture Organization of the United Nations (FAO), livestock vaccination is ongoing. In total 338 000 doses of anthrax vaccine have been distributed up to 19 November 2023. Vaccination campaigns have been initiated at the outbreak epicentre, Sinazongwe district, and is extended to other affected districts. A joint One Health task force comprising the Ministry of Health and the Ministry of Local Government has been conducting case finding in animals and humans. Meat inspection is enhanced by the veterinary department. Additionally, the Department of Wildlife and Parks has been actively involved, conducting patrols to monitor illegal animal movements and ensuring proper disposal of carcasses. WHO is working closely with FAO and the Ministry of Agriculture on animal health activities like vaccination.
Actions implemented for humans
WHO is supporting and working closely with the Ministry of Health in the following activities.
For case management, health workers have undergone orientation to enhance their capacities to identify potential cases early on. Efforts have been made to strengthen event-based surveillance (EBS) and early detection mechanisms. Provision of essential medical supplies has been prioritized, in addition to public sensitization. Active surveillance is ongoing across healthcare facilities and within communities, including contact tracing.
Meat inspections are being conducted in abattoirs and butcher shops. Preparedness plans are in place, including the mobilization of additional healthcare personnel to districts, foreseeing a potential surge in anthrax cases. Moreover, specialized training sessions for provincial practitioners aim to improve case management proficiency in the provinces.
The laboratory continues to operate under a unified One Health approach for diagnostics. Procurement efforts for laboratory reagents are underway due to shortages. Strict protocols for disinfection and decontamination remain ongoing to ensure safety.
Extensive health promotion and Risk Communication and Community Engagement (RCCE) activities are ongoing, including press briefings by Ministry of Health, social media campaigns, radio broadcasts, and the distribution of informative brochures and posters.
WHO Risk Assessment
Anthrax is endemic in Zambia, usually occurring between May and January, with a peak toward the end of the dry season (between October and November). Although sporadic cases are reported yearly in animals and humans across the country, a large-scale outbreak like the current one has not been reported since 2011, when there were 511 suspected human cases.
The epidemic is spreading along the provinces located along the basin of the Zambezi, Kafue, and Luangwa rivers, which is an additional problem because these rivers also flow into Lake Kariba in Zimbabwe, Kahora Bassa in Mozambique and Lake Malawi, and the risk of anthrax transmission to neighbouring countries is increased.
Other affected districts and provinces of Zambia have reported sporadic suspected cases and deaths since June 2023. In addition, the Bacillus anthracis bacteria can form highly resistant spores that survive in the environment for decades
The risk for human health is high given the known population’s multiple exposures from handling the carcasses of animals that had died suddenly and eating meat from infected animals with resultant associated cutaneous and gastrointestinal anthrax.
The risk of the event spreading within Zambia has increased due to the unrestricted animal movement and carcasses within and between provinces. Since September 2023, there has been a significant rise in the number of affected districts. Moreover, a low index of suspicion, socio-cultural norms, community resistance, limited community knowledge regarding anthrax transmission, high levels of poverty and food insecurity, a shortage of available vaccines and laboratory reagents, inadequate carcass disposal and decontamination practices significantly contribute to hampering the containment of the anthrax outbreak.
There is an absence of robust engagement with local communities involved in breeding and handling cattle and livestock, including farmers, heads of cattle markets, and butchers. Among these communities, the fear of losing livelihoods often outweighs concerns about contracting anthrax. The risk of insufficient control capacities is considered high in Zambia due to concurrent public health emergencies in the country (cholera, measles, COVID-19) that limit the country’s human and financial capacities to respond to the current anthrax outbreak adequately.
The risk at the regional level is also considered high due to the frequent movement of both animals and people between Zambia and its neighbouring countries (such as Angola, Botswana, the Democratic Republic of the Congo, Malawi, Mozambique, Namibia, Tanzania, Uganda and Zimbabwe). This is compounded by the confirmed cases of anthrax spreading in provinces located along the basin of the Zambezi, Kafue, and Luangwa rivers. These rivers ultimately flow into Lake Kariba in Zimbabwe, the Kahora Bassa lake in Mozambique, and Lake Malawi.
Unburied carcasses of wild animals that float on the river increase the risk of international spread to neighbouring countries. They can spread the bacterium and infections to other regions, including neighbouring countries, and be eaten by other animals, which can further perpetuate the spread.
WHO Advice
Humans usually acquire the infection after exposure to infected animals, carcasses, or animal products. More than 95% of human anthrax cases take the cutaneous form and result from handling infected carcasses or hides, hair, meat or bones from such carcasses. The public should avoid handling and consumption of meat from animals that died suddenly, meat obtained via emergency slaughter, and meat of uncertain origin. Anthrax can also be an occupational hazard for veterinarians, agriculture and wildlife workers, or workers who butcher animals or process meat, hides, hair, and wool and should wear preventive clothing and gloves or personal protection equipment (PPE).
In health-care settings, it is crucial to enhance screening procedures specifically in areas where there is a known epidemiological risk of anthrax. It is imperative to anticipate and implement infection prevention and control measures promptly when cases are suspected. When caring for patients with draining anthrax lesions, implementing contact precautions is vital. This includes placing the patient in a private room and the use of PPE (such as examination gloves and a fluid resistant gown). Additionally, dressings may be used to contain drainage and reduce the risk of environmental contamination. These dressings should be disposed of as infectious waste after use. The WHO’s 5 Moments for hand hygiene should be practiced using soap and water when caring for suspected and confirmed cases, as alcohol-based hand rub has weakened effect against spores. For areas where patients with suspected or confirmed exposure to anthrax spores are being cared for, it is recommended to implement enhanced cleaning and disinfection protocols.
Individuals potentially exposed to anthrax spores should receive prophylactic treatment. Anthrax responds well to antibiotics, which need to be prescribed by a medical professional. Strict adherence to the full course of treatment is vital. Human vaccines are in limited supply and used primarily for the protection of selected individuals with possible occupational exposure to anthrax.
International travelers to anthrax endemic countries should be aware of regulations concerning the importation of prohibited animal products, trophies, and souvenirs.
Anthrax is controlled through animal vaccination programs, rapid detection and reporting, quarantine, treatment of sub clinically affected animals (postexposure prophylaxis) and burning or burial of suspect and confirmed animal cases. The carcass should not be opened since exposure to oxygen will allow the bacteria to form spores. The general public and at-risk individuals should immediately report instances of sick or unexpected deaths in animals to veterinary authorities. Veterinary vaccines are used for control of anthrax in livestock. Vaccination protocols for livestock should be strictly followed to curb anthrax spread. Preventing the disease in animals will protect human health.
WHO advises against implementing any travel or trade restrictions based on the current information available on this event.
Further Information
- Ministry of health of Zambia. Press statement on Anthrax, 1 November 2023. Available from https://www.moh.gov.zm
- Ministry of Health in Malawi. Press release. 3 November 2023. https://www.facebook.com/photo/?fbid=647772487535028&set=a.234388385540109
- World Health Organization, United Nations Food and Agriculture Organization, World Organisation for Animal health. Anthrax in humans and animals – 4th ed, Geneva Switzerland: World Health Organization; 2008. Available from: https://www.who.int/publications/i/item/9789241547536
- World Health Organization. Guidelines for the surveillance and control of Anthrax in humans and animals – 3rd ed, Geneva Switzerland: World Health Organization; 1998. Available from https://www.who.int/publications/i/item/guidelines-for-the-surveillance-and-control-of-anthrax-in-humans-and-animals
- World Health Organization. Anthrax questions and answers, 18 November 2016. Available from: https://www.who.int/europe/news-room/questions-and-answers/item/anthrax
- World Health Organization. Standard precautions for the prevention and control of infections: aide-memoire. Available from: https://www.who.int/publications/i/item/WHO-UHL-IHS-IPC-2022.1
- World Health Organization. Transmission-based precautions for the prevention and control of infections: aide-memoire. Available from: https://www.who.int/publications/i/item/WHO-UHL-IHS-IPC-2022.2
- World Organisation for Animal Health. Report preview-Zambia-Anthrax-immediate notification, 2023. Available from: https://wahis.woah.org/#/in-review/5329
- FAO: Stopping an anthrax outbreak through One Health in Zambia. Available from: https://www.fao.org/africa/news/detail-news/en/c/1653125/
- Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of High-Consequence Pathogens and Pathology (DHCPP).
- What is Anthrax, United States of America: CDC; 2022. Available from https://www.cdc.gov/anthrax/basics/index.html
Citable reference: World Health Organization (8 December 2023). Disease Outbreak News; Anthrax in Zambia. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON497







{kind=link}