
Malawi is experiencing a widespread cholera outbreak, with 36 943 cases and 1210 associated deaths reported from all 29 districts since 3 March 2022. This is the deadliest outbreak of cholera in the country’s history.
Cholera has been endemic in Malawi since 1998 with seasonal outbreaks reported during the rainy season (November through May). However, the current outbreak has extended through the dry season, with cases being reported since March 2022.
In light of the ongoing rainy season, wide geographical spread, and a consistently high case fatality rate (CFR) of above 3%, the ongoing cholera outbreak was declared a public health emergency by the Malawi government on 5 December 2022. Currently, the large geographic spread and the high number of reported cases in the country are stretching all capacity to respond to the outbreak, increasing the risk of serious public health impact. The outbreak in Malawi is occurring against a backdrop of a surge in cholera outbreaks globally, which has constrained the availability of vaccines, tests, and treatments.
With a sharp increase of cases seen over the last month, fears are that the outbreak will continue to worsen without strong interventions.
Description of the cases
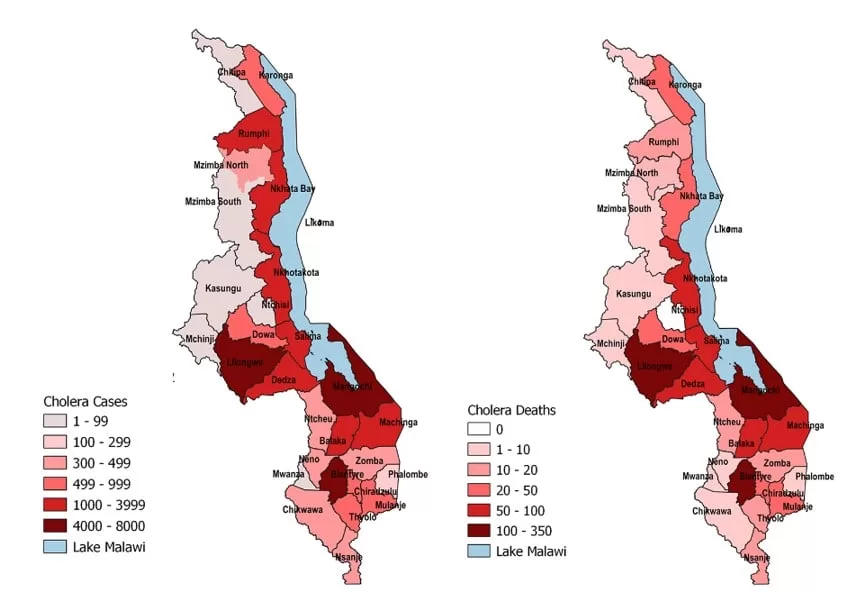
Between 3 March 2022 through 3 February 2023, a total of 36 943 cases, including 1210 deaths, have been reported from all 29 districts in Malawi (overall case fatality rate (CFR) 3.3%) with active transmission ongoing in 27 of 29 districts. There was a 143% increase in the number of cases in January (17 078) compared to December (7017 cases). As of 3 February, Mangochi district bordering Lake Malawi is the most affected area, reporting 6974 cases and 114 deaths (CFR 1.6%).
The current outbreak started in March 2022 from Machinga district following tropical storm Ana (January 2022) and Cyclone Gombe (March 2022) which caused floods leading to the displacement of a population with low pre-existing immunity and had lack of access to safe water, sanitation, and hygiene. The outbreak was mainly limited to the flood-affected areas in the southern region until August 2022 when it spread to the northern and central parts of the country. Since December 2022 cases have spread back towards the south of the country with all regions affected including Blantyre and Lilongwe, the two main cities of the country.
Since the beginning of the outbreak, and as of 3 February 2023, the age group 21 to 30 years is the most affected (27.7% of cases) followed by the 11 to 20 age group (22.8%). Of all the cases,17 943 are males representing 57% of the caseload. Most deaths have been reported among those aged 60 years and above as of 29 January 2023. Most deaths have occurred among males (66%).
From 1998 to date, cholera cases have been reported in the country, especially in the southern region, which is low-lying, flat, and prone to flooding during the rainy season. The highest numbers of cases and deaths were reported in 1998/99 (25 000 cases, 860 deaths, CFR 3.4%), 2001/02 (33 546 cases, 968 deaths, case fatality rate 2.3%), and 2008/09 (5751 cases, 125 deaths, CFR 2.2%).
Figure 1: Number of suspected and confirmed cholera cases (n=36 943) and deaths (n=1210) per day in Malawi, 3 March 2022 to 3 February 2023.

Source: Malawi Ministry of Health and Population
Figure 2: Geographical distribution of confirmed and suspected cholera cases (n=36 943) and deaths (n=1210) by District in Malawi, 3 March 2022 to 3 February 2023.

Source: Malawi Ministry of Health and Population
Figure 3. Age-sex distribution of confirmed and suspected cholera cases (n=36 943) in Malawi, 3 March 2022 to 3 February 2023.

Source: Malawi Ministry of Health and Population
Epidemiology of Cholera
Cholera is an acute enteric infection caused by ingesting the bacteria Vibrio cholerae present in contaminated water or food. It is mainly linked to inadequate sanitation and insufficient access to safe drinking water. It is an extremely virulent disease that can cause severe acute watery diarrhoea resulting in high morbidity and mortality, and can spread rapidly, depending on the frequency of exposure, the exposed population and the setting. Cholera affects both children and adults and in its’ severe form can be fatal within hours if untreated.
The incubation period is between 12 hours and five days after ingestion of contaminated food or water. Most people infected with V. cholerae do not develop any symptoms, although the bacteria are present in their faeces for 1-10 days after infection and are shed back into the environment, potentially infecting other people. Most people who develop symptoms have mild or moderate symptoms, while a minority develop severe forms of the disease with acute watery diarrhoea and vomiting leading to severe dehydration. Cholera is an easily treatable disease. Most people can be treated successfully through prompt administration of oral rehydration solution (ORS) and successful rehydration therapy can keep the CFR below 1%.
The consequences of a humanitarian crisis – such as disruption of water and sanitation systems, or the displacement of populations towards inadequate and overcrowded camps – can increase the risk of cholera transmission, should the bacteria be present or introduced.
A multi-sectoral approach including a combination of surveillance, water, sanitation and hygiene (WASH), social mobilization, treatment, and oral cholera vaccines is essential to control cholera outbreaks and to reduce deaths.
Public health response
Emergency response activities are being conducted by the Ministry of Health, WHO and other partners since the declaration of the outbreak in March 2022.
Coordination and response:
- The ongoing cholera outbreak has been declared a public health emergency by government of Malawi on 05 December 2022. This led to the incorporation of cholera into its Presidential Taskforce on Coronavirus Disease, to be responsible for coordination of the outbreak response. The Presidential Task Force members on COVID-19 and cholera have been visiting all affected district to understand the situation.
- A costed national cholera response plan to manage the outbreak was drafted and is being updated regularly. WHO and other partners are supporting the implementation of various activities aligned with the plan. National- and district-level emergency operation centres (EOCs) have been operationalized to coordinate the multisectoral response with other partners.
- Multisectoral coordination group for cholera response has been established in the affected districts.
- The National Incident Management Team (IMT) continues to coordinate technical response to the outbreak. The IMT meets twice a week at the Public Health Emergency Operations Centre (PHEOC) in Lilongwe. The WHO IMT team is meeting three times a week for updates in between the National IMT to coordinate how to provide support efficiently across all response pillars.
- All technical thematic areas led by the Ministry of Health with support from WHO and partners continue to routinely provide technical support and coordinate field-level implementation.
- Cross-border preparedness is ongoing, with meetings held by health officials from MOH, WHO and Partners in Mozambique and Zambia through inter-district committees.
Surveillance:
- National rapid response teams (RRT) have been deployed to all the affected districts.
- Health Surveillance Assistants have been trained on active case investigation and surveillance.
- Detection of cases at community and health facilities levels continue. Rapid response team established in each districts continue to investigate cases.
- Data collection and analysis is ongoing, and situation reports are being produced and published regularly. Deep-dive epidemiological analysis of the cholera situation is ongoing.
- Data collection tools have been harmonized, printed and distributed to all districts. More tools are being printed to meet the rising demand of reporting with the high volume of cases.
- The Ministry of Health with support from WHO and partners have strengthened community-based surveillance for early detection of cases through the utilization of community health volunteers. Lilongwe district which is one of the most affected districts has initiated integrated community interventions to interrupt transmission and reduce cholera-related deaths. The same interventions have been implemented in six high-burden districts and then rolled out across all the districts.
- Joint Ministry of Health and WHO field operational visits are ongoing in districts with high case load and deaths.
- The recruitment and deployment of surveillance officers and data analysts in high-burden districts to improve reporting and data quality is ongoing.
- Currently a team of local and international surge staff is in country to support strengthening of information management, surveillance and data management. The team continues to produce information products in form of daily and weekly situation reports, maps detailing case and mortality burden, location of cholera treatment centers (CTCs)/ cholera treatment units (CTUs), profiling of deaths by age group, location and treatment facilities they are occurring to guide targeted interventions.
Health System Strengthening/Case Management:
- Case management was initially conducted through very large numbers (345) of cholera treatment units (CTUs) across all affected districts. As the extent and geography of cases has become clearer, this has been rationalised, with fewer centres. This presents an opportunity to strengthen the quality of care while respecting the decentralised approach. In some areas of high need, new structures have been set up or expanded (for example Bwaila and Area 25 in Lilongwe).
- Review and assessment of CTUs has been conducted across four regions in the last week (Salima, Blantyre, Lilongwe, Balaka), and more than 20 sites, with immediate needs identified and logistical input sought. This included the establishment of improved water and electricity supplies, improved waste management, and provision of beds and medical equipment for dealing with critical illness.
- Staff training has included, in collaboration with partners and Ministry of Health, 13 doctors, 46 trainer-of-trainers, and approximately 200 nursing staff ready to deploy to areas of need.
- Core standardised materials for patient care have been created and agreed with the MoH to enable the recording of treatment and response (including fluids and observation charts).
- To establish patient-level data to inform on care quality and to enhance our understanding of cholera presentations, a paper and electronic data capture form has been agreed with MoH, and begun to be deployed to CTCs.
- A network of supportive supervision from the tertiary hospitals has been created, with provision for outreach from specialist centres into patient treatment areas in order to enhance quality of care delivered, and support CTU staff.
- Partner and centre mapping continues, with the identification of formal and informal referral pathways. This includes those from high-burden areas, and specific demographics (e.g. under 2-year-olds), and has informed the strengthening of CTC staff numbers.
- WHO and partners supporting the establishment of oral rehydration points (ORPs) in high burden communities, inclusive of area 25, area 18, Likuni and Bwaila communities. Currently, 47 (ORPs) have been established in 10 high burden districts to serve as primary care points for cases in the communities. Church leaders, chieves, village headmen and community health workers and volunteers were orientated on the operation of ORPs and emphasis on their community engagement. The provision of ORPs needs to be scaled rapidly to provide early intervention and avoid admission with severe dehydration.
- Supportive supervision visits are being conducted on infection prevention and control and water, sanitation, and hygiene in CTCs in three districts. Main areas mentored on include patient segregations according to severity of disease during care in the CTC, handling of inserted devises, waste management, linen management, management of chlorine, use of personal protective equipment (PPE), management of guardians, and environmental cleaning.
- The teams also visited three communities in the three districts to assess WASH, including sanitary inspections of water sources, sanitation facilities, safe water accessibility, household water chlorination and conducted health education in communities.
Capacity Building/IPC:
- Training of trainees has been conducted on cases management in Nkhotakota, Rumphi, Likoma, Chitipa, Nkhatabay, Mzimba North, Mzimba South and Karonga.
- Ongoing community field visits to assess WASH, including sanitary inspections of water sources, sanitation facilities, safe water accessibility, household water chlorination and conducted health education in communities.
- On-site IPC training and mentorship has been conducted amongst health care workers in CTCs/CTUs across all the districts in Northern Districts.
Human Resource:
- Ministry of Health has advertised on recruitment of surge staff to support cholera response in the districts Blantyre, Karonga, Lilongwe, Mangochi, Nkhatabay, Nkothakota, Rumphi, and Salima.
- WHO is supporting the recruitment of 40 medical doctors (21 already reported for duty as of 03 February 2023), 80 clinical technicians and 160 nurses to support in the CTCs/CTUs across the country.
Laboratory:
- WHO is supporting the Ministry of Health in increasing laboratory testing capacity and diagnostics to continue to monitor incidence in all affected areas with a focus on early detection and confirmation of new cases in unaffected areas, as well as genomic sequencing of Vibrio cholerae.
- The WHO is supporting capacity building, provision of reagents, and standard operating procedures.
- Collection of samples for sequencing is ongoing. Meanwhile, periodic testing of cases is being done with 5-10 samples being collected systematically every week from CTCs/CTUs.
Logistics and Supplies:
- Cholera kits and other supplies including oral rehydration salt, IV Fluids, antibiotics, rapid diagnostic test kits, personal protective equipment, tents, and cholera beds have been provided by WHO and partners in affected districts.
- Treatment structures and ORS points have been established in the affected districts. Currently, 345 CTC and CTUs were established with 140 being active, and 47 ORPs set up in 10 districts serving over 180 000 population at high risk.
- WHO has provided cholera kits and other supplies which are being distributed to the affected districts, supporting 48 000 cholera cases since the beginning of the outbreak. Additional supplies are being mobilized.
- As of 03 February 2023, 35 cholera kits (drug module) composed of 17 600 litres of ringers are in shipment to arrive in country.
- 1271 ringers lactate (500 ml) and 5300 bags of ORS have been dispatched by WHO to District Hospitals with a high burden of disease including Lilongwe.
Reactive Vaccination Campaigns:
Two oral cholera vaccine (OCV) vaccination campaigns have been conducted across 21 districts since the onset of the outbreak.
- Following a request for OCV to the International Coordinating Group on Vaccine Provision (ICG) and approval in May 2022, a total of 1 947 696 doses were received as the first batch. Reactive vaccination campaign for one round of OCV was implemented in eight districts including Balaka, Blantyre, Chikwawa, Machinga, Mangochi, Mulanje, Nsanje and Phalombe between 23 through 27 May 2022. The cumulative vaccination coverage achieved was 69%.
- A second request for OCV was submitted to the ICG in October 2022, and 2 941 982 doses were approved for a single dose campaign. The campaign was implemented from 28 November through 2 December 2022 in 13 districts: Chitipa, Kasungu, Nsanje, Rhumphi, Salima, Karonga, Zomba, Mzimba North and South, Nkhatabay, Nkhotakota, Lilongwe, Likoma. The cumulative coverage achieved was 83.6%.
- Ongoing provision of OCV continued beyond the campaign period with additional campaigns in Mangochi and Blantyre (beyond the 13 targeted district). In total, 96.8% (2 825 229 doses) of the population residing in communities with high risk and burden of cholera were reached with OCV.
Risk Communication and Community Engagement:
- Community and national radios are being used for spreading awareness in the affected communities and spreading message for cholera prevention. Four community radios (Nkhotakota, Nkhatabay, Mzimba and Rumphi) produced jingles, airing radio programs and live panel discussion with support from UNICEF.
- WHO has supported the creation of Information, education and communication materials (WASH cholera brochure, cholera poster, leaflet for health workers, posters on waste management, OCV campaign posters).
- Local leaders and health-based leaders have been engaged by health promotion officers with support from Red Cross.
- Districts authorities have been communicated to write letters to churches, chiefs and local community structures to strengthen cholera prevention measures in the community and during gatherings.
- Knowledge, Attitude and Perception survey has been conducted in Blantyre, Salima Nkhatabay to understand the drivers of the cholera outbreak and guide targeted interventions in the affected communities.
WASH Interventions:
- Provision of mobile latrines in the cholera treatment camps and installation of prefabricated latrines in five camps.
- Households in the affected districts are being sensitized on WASH promotion including water treatment and hand hygiene.
- House-to-house chlorination is ongoing in affected communities in all the districts.
- Water quality monitoring tests have been donated by UNICEF and have been distributed across the districts to strengthen water quality surveillance.
- Water quality surveillance have been conducted in Balaka, Blantyre, Chikwawa, Karonga, Machinga, Mangochi, Mwanza, Neno, Nsanje, Mwanza, Salima, Nkhotakota, and Nkhatabay.
- Supply of High-Test Hypochlorite by The Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) to Nkhotakota, Nkhatabay, Rumphi, Karonga and Mzimba
- A total of 9579 chlorine dispensers have been installed in four districts including Zomba, Blantyre, Balaka and Mangochi.
- Continued distribution of 1% stock solution is being done to community members in all districts by Health Surveillance Assistants.
WHO risk assessment
Cholera is endemic in Malawi with seasonal outbreaks occurring during the wet season. The first major outbreak occurred in 1998 and was widespread in the Southern Region, with 25 000 cases reported. Prior to the current outbreak, the largest outbreak in Malawi occured from October 2001 to April 2002, and affected 26 of the 29 districts, with 33 546 cases and 968 deaths (CFR 3%).
Following floods in the southern region in January 2022, the Ministry of Health confirmed a cholera outbreak on 3 March 2022. This outbreak, which was initially limited to the Southern Region and the flood-affected areas, has now spread to all the regions and districts in the country. Transmission has continued during the dry season (June to October), which is traditionally a low transmission period for Malawi. With the onset of the rainy season from November through May, the number and spread of cholera cases is expected to increase further. Therefore, the risk is considered to be very high at the national level. The poor WASH capacities in the affected districts, especially in the fishing communities along Lake Malawi, pose risk for the continuous propagation of the cholera outbreak nationally, to neighbouring countries and in the region.
Two reactive single-dose OCV campaigns have been carried out in parts of 21 affected districts, however unvaccinated sub-districts and districts still remain at risk. Other identified challenges from the most at-risk districts include inadequate capacity for case management and diagnosis in the affected areas resulting in delayed case detection and poor outcomes. This is further exacerbated due to delayed care-seeking behaviour of the community.
There is a continued risk for further increase in the number of cases and international spread. Confirmed cases have been reported across the border in Mozambique and the risk for cross-border transmission between Malawi and Mozambique remains high during the current outbreak.
The country has experience in controlling cholera outbreaks. However, due to concurrent outbreaks (polio, COVID-19), the large geographic spread of the outbreak (with cases reported in all districts) and the high case numbers, the current burden is overstraining existing national response capacity and resources as well as the capacity of partners’ support. In addition, there are multiple ongoing large cholera outbreaks worldwide. This is stretching limited global stocks of cholera supplies and OCV, which limits available resources for Malawi and the region.
WHO assesses the risk of this outbreak to be very high at national and regional level. On 21 January 2023, WHO assessed the risk of the global cholera outbreak as very high due to ongoing multiple cholera outbreaks in many WHO regions.
WHO advice
There is an urgent need to improve access to safe water sanitation and hygiene. WHO recommends improving access to safe drinking water and sanitation infrastructure, improving access to proper and timely case management of cholera cases as well as improving infection, prevention, and control in healthcare facilities. Promotion of preventive hygiene practices and food safety in affected communities are the most effective means of controlling cholera. Targeted public health communication messages are a key element for a successful response. OCV should be used in conjunction with improvements in water and sanitation to control cholera outbreaks and for prevention in targeted areas known to be at high risk for cholera.
One of the factors contributing to the high CFR in Mangochi, Blantyre, Machinga, Lilongwe was late presentation to a health facility. Delay in health-seeking behaviour, and limited community sensitization can lead to treatment delays and increased deaths, as well as an underestimation of the scale of the outbreak (cases and related deaths). WHO recommends Member States to strengthen and maintain surveillance for cholera, especially at the community level, for the early detection of suspected cases and to provide adequate treatment and prevent its spread. Early and adequate treatment limits the CFR of hospitalized patients to less than 1%. Inter-district and cross-border coordination and collaboration, risk communication, and community engagement are crucial in the prevention and containment of this cholera outbreak.
WHO does not recommend any travel or trade restrictions on Malawi based on the currently available information. However, as the outbreak is taking place in border areas where there is a significant cross-border movement, WHO encourages Malawi and its neighbouring countries to ensure cooperation and regular information sharing so that any spread across the border is quickly contained.
Further information
- WHO Cholera fact sheet
- Weekly Epidemiological Record 2016
- Weekly Epidemiological Record 2017
- Weekly Epidemiological Record 2019
- Weekly Epidemiological Record 2020
- Weekly Epidemiological Record 2021
- UNICEF Situation Report – Malawi floods, published on 17 March 2022: https://www.unicef.org/malawi/media/6941/file/Malawi%20Floods%20Humanitarian%20Situation%20Rep%20ort%2017%20March%202022.pdf
- Tropical storms, flooding and Cholera: Malawi faces cholera emergency amidst severe climate events, published on 23 March 2022: https://www.afro.who.int/photo-story/tropical-storms-flooding-and-cholera-malawi-faces-cholera-emergency-amidst-severe
- WHO cholera fact sheet, published on 30 March 2022: http://www.who.int/news-room/factsheets/detail/cholera
- WHO Disease Outbreak News: Cholera in Malawi, published on 27 April 2022: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON372
- WHO Africa – Malawi News: UNICEF and WHO step up efforts to contain Cholera in Malawi and call for additional funds and support published on 24 August 2022: https://www.unicef.org/malawi/press-releases/unicef-and-who-step-efforts-contain-cholera-malawi-and-call-additional-funds-and
- WHO Disease Outbreak News: Cholera in Malawi, published on 7 November 2022: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON419
- Malawi Ministry of Health Cholera Surveillance Dashboard https://public.tableau.com/app/profile/phimcholeradashboard/viz/CholeraDashboard/EPICurveS
Citable reference: World Health Organization (9 February 2023). Disease Outbreak News; Cholera – Malawi. Available at https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON435







{kind=link}