
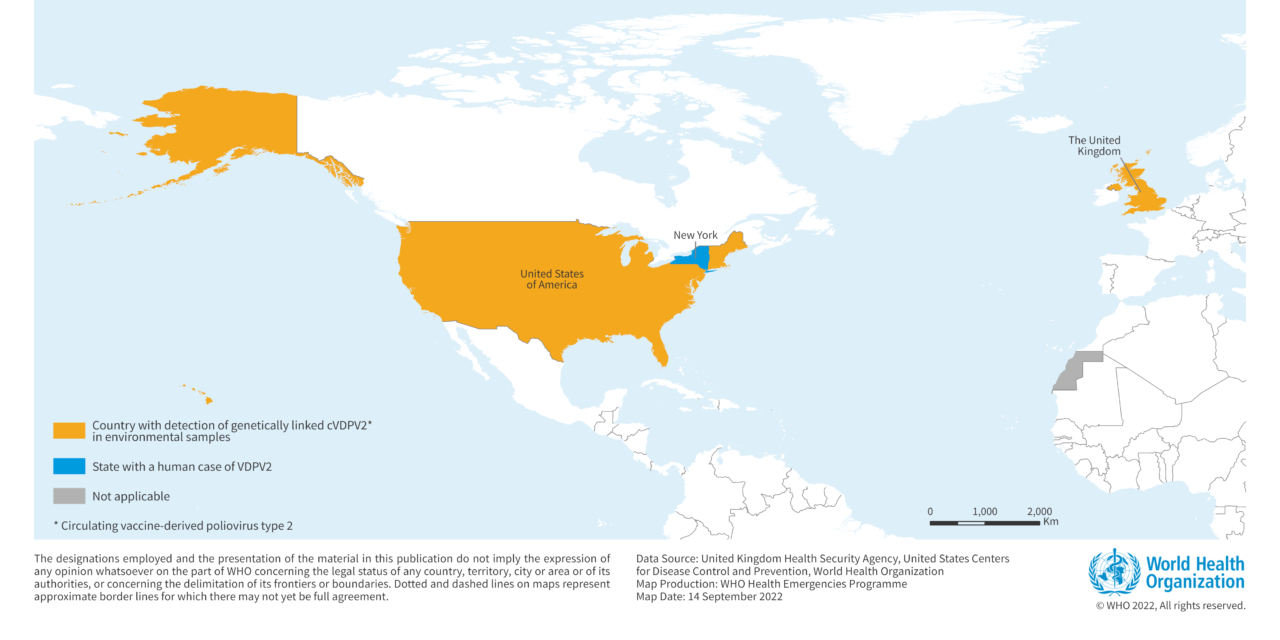
Figure-1 Detection of genetically linked cVDPV2 isolates in the United Kingdom and the United States of America from February to August 2022

Epidemiology of Poliomyelitis
Polio is a highly infectious disease that largely affects children under five years of age, causing permanent paralysis (approximately 1 in 200 infections) or death (5-10% of those paralyzed).
The virus is transmitted from person-to-person, mainly through the fecal-oral route or, less frequently, by a common vehicle (e.g., contaminated water or food) and multiplies in the intestine, from where it can invade the nervous system and cause paralysis and death. Initial symptoms of polio include fever, fatigue, headache, vomiting, stiffness of the neck and pain in the limbs. In a small proportion of cases, the disease causes paralysis, which is often permanent. There is no cure for polio but it can be prevented by immunization.
The incubation period is usually 7–10 days but can range from 4–35 days. Up to 90% of those infected are either asymptomatic or experience only mild symptoms and the disease often goes unrecognized.
Vaccine-derived poliovirus is a well-documented type of poliovirus that has mutated from the strain originally contained in the oral polio vaccine (OPV). The OPV contains a live, weakened form of poliovirus. On rare occasions, when replicating in the gastrointestinal tract, OPV strains genetically change and may spread in communities that are not fully vaccinated against polio, especially in areas where there is poor hygiene, poor sanitation, or overcrowding. Further changes occur as these viruses spread from person to person. The lower the population immunity, the longer this virus survives and the more genetic changes it undergoes. In very rare instances, the vaccine-derived virus can genetically change into a form that can paralyze – this is what is known as a vaccine-derived poliovirus (VDPV).
The detection of VDPV in at least two different sources and at least two months apart, that are genetically linked, showing evidence of transmission in the community, should be classified as ‘circulating’ vaccine-derived poliovirus type 2 (cVDPV2). cVDPV2 continues to affect different areas of the world.
Public health response
- Public health measures in the United Kingdom
The United Kingdom Health Security Agency (UKHSA) is conducting further investigations including assessing the public health risk and implementing response measures. These measures include:
- Strengthening the environmental, clinical and laboratory surveillance for polio.
- A catch-up campaign targeted at children aged less than 5 years of age in London was implemented in June 2022, and a supplementary booster inactivated polio vaccine (IPV) campaign targeting children aged 1 to 9 years in London was launched in August 2022.
- Public health professionals, health professionals, and laboratory staff alerted to the detection of VDPV2 in London.
- Health professionals reminded of the importance of checking newly registered children and adult routine immunizations are up-to-date, with an emphasis on under-immunized populations (new migrants, asylum seekers and refugees).
- Local and regional laboratories requested to refer all enterovirus positive stool samples to the UKHSA.
- Enhancing environmental sampling to assess the extent of the spread of the virus across London. In addition, a range of additional sewage sampling sites are being stood up across the country.
- Public health measures in the United States of America
- Enhancing polio wastewater surveillance.
- Ongoing activities to support polio vaccination and increase vaccination coverage in Rockland and Orange Counties in New York State. Planning underway to launch an immunization campaign to provide IPV to residents of Rockland County who have potentially been exposed to poliovirus.
- Conducting testing for poliovirus in wastewater samples in New York and neighbouring States, as well as providing confirmatory testing for clinical specimens.
- Coordinating surveillance for Acute Flaccid Myelitis (AFM) throughout the United States of America and enhancing surveillance for paralytic and non-paralytic polio in areas where poliovirus has been detected in wastewater.
- Health advisories including information on polio, the situation in New York State, and polio immunization, have been released to health providers and hospitals across the State and in the immediate county of residence of the case.
- On 9 September, a state disaster emergency due to polio was declared in New York State. The declaration allows additional health professionals, such as pharmacists, to administer polio vaccine and allows health practitioners to issue standing orders for polio vaccinations.
WHO risk assessment
The emergence of cVDPV2 in the United Kingdom and in the United States of America is a reminder that until polio is eradicated, polio-free countries will remain at risk of polio re-infection or re-emergence. The detection of this VDPV2 strain underscores the importance of;
Based on the WHO UNICEF estimates, the vaccine coverage for three routine doses of polio vaccine evaluated in children aged 12 months in the United Kingdom and United States of America were 93% and 92% respectively in 2021.
WHO will continue to support the ongoing investigation, risk assessment and outbreak response by national authorities.
WHO advice
WHO reiterates to all Member States the importance of reaching and maintaining polio vaccination coverage of more than 95% in each district or municipality; maintaining high quality for three main surveillance indicators: acute flaccid paralysis (AFP) rate, percentage of cases investigated within 48 hours, and percentage of cases with an adequate sample; optimizing supplementary (environmental and enterovirus) poliovirus surveillance and updating national poliovirus outbreak response plans in order to rapidly detect and respond to new virus importations or VDPV emergence to minimize the consequences of poliovirus transmission and facilitate a rapid response.
The thirty-second polio IHR Emergency Committee meeting held in June 2022, convened under the International Health Regulations (2005), agreed that the risk of international spread of poliovirus remains a Public Health Emergency of International Concern (PHEIC) and recommended the extension of Temporary Recommendations for a further three months.
Further information
- Global Polio Eradication Initiative: http://polioeradication.org/
- Polio Factsheet: https://www.who.int/health-topics/poliomyelitis#tab=tab_1
- WHO/UNICEF estimates of national routine immunization: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage
- GPEI Public health emergency status: http://polioeradication.org/polio-today/polio-now/public-health-emergency-status/
- International travel and health: https://www.who.int/ith/en/
- Vaccine-derived polioviruses: http://polioeradication.org/polio-today/polio-prevention/the-virus/vaccine-derived-polio-viruses/
- Standard operating procedures: responding to a poliovirus event or outbreak, version 3.1. POL-SOP-V3.1-20200424.pdf(polioeradication.org)
- Guidance on Inactivated polio vaccine (IPV) booster campaign: information for healthcare practitioners, updated 11 August 2022, UK health security agency: https://www.gov.uk/government/publications/inactivated-polio-vaccine-ipv-booster-information-for-healthcare-practitioners/inactivated-polio-vaccine-ipv-booster-campaign-information-for-healthcare-practitioners#ref
- Cover of vaccination evaluated rapidly (COVER) programme 2021 to 2022: quarterly data: https://www.gov.uk/government/statistics/cover-of-vaccination-evaluated-rapidly-cover-programme-2021-to-2022-quarterly-data
- Joint Committee on Vaccination and Immunisation statement on vaccination strategy for the ongoing polio incident, published on 10 August 2022, https://www.gov.uk/government/publications/vaccination-strategy-for-ongoing-polio-incident-jcvi-statement/joint-committee-on-vaccination-and-immunisation-statement-on-vaccination-strategy-for-the-ongoing-polio-incident
- Vaccine-derived poliovirus type 2 detected in environmental samples in London: https://polioeradication.org/news-post/vaccine-derived-poliovirus-type-2-vdpv2-detected-in-environmental-samples-in-london-uk/
- Circulating Vaccine-Derived Poliovirus type 2 (cVDPV2) in the United Kingdom: https://polioeradication.org/where-we-work/united-kingdom/
- Polio detection in the United States of America: https://polioeradication.org/news-post/report-of-polio-detection-in-united-states/
- Weekly epidemiological update on Polio: https://polioeradication.org/polio-today/polio-now/this-week/
- Pan American Health Organization / World Health Organization. Epidemiological Alert. Detection of vaccine-derived poliovirus type 2 (VDPV2) in the United States: Implications for the Region of the Americas. 21 July 2022, Washington, D.C.: PAHO/WHO; 2022: https://www.paho.org/en/documents/epidemiological-alert-detection-vaccine-derived-poliovirus-type-2-vdpv2-united-states
- Pan American Health Organization / World Health Organization. Epidemiological Alert. Poliovirus outbreak risk. 10 June 2022, Washington, D.C.: PAHO/WHO; 2022: https://www.paho.org/en/documents/epidemiological-alert-poliovirus-outbreak-risk-10-june-2022
- Center for Disease, Control and Prevention (US CDC). Public Health Response to a Case of Paralytic Poliomyelitis in an Unvaccinated Person and Detection of Poliovirus in Wastewater — New York, June–August 2022: https://www.cdc.gov/mmwr/volumes/71/wr/pdfs/mm7133e2-H.pdf
- WHO/UNICEF estimates of national routine immunization: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage
- Center for Disease, Control and Prevention (US CDC). United States confirmed as country with circulating vaccine-derived poliovirus: https://www.cdc.gov/media/releases/2022/s0913-polio.html
- Gelles R, Lutterloh E, Schnabel Ruppert P, et al. Public Health Response to a Case of Paralytic Poliomyelitis in an Unvaccinated Person and Detection of Poliovirus in Wastewater — New York, June–August 2022. MMWR Morb Mortal Wkly Rep 2022;71:1065-1068. DOI: http://dx.doi.org/10.15585/mmwr.mm7133e2
Citable reference: World Health Organization 14 September 22 2022). Disease Outbreak News; Detection of circulating vaccine derived polio virus 2 (cVDPV2) in environmental samples– the United Kingdom of Great Britain and Northern Ireland and the United States of America . Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON408
[1] No further information is available on VDPV2 detections in Israel at this stage as investigations are ongoing









{kind=link}