
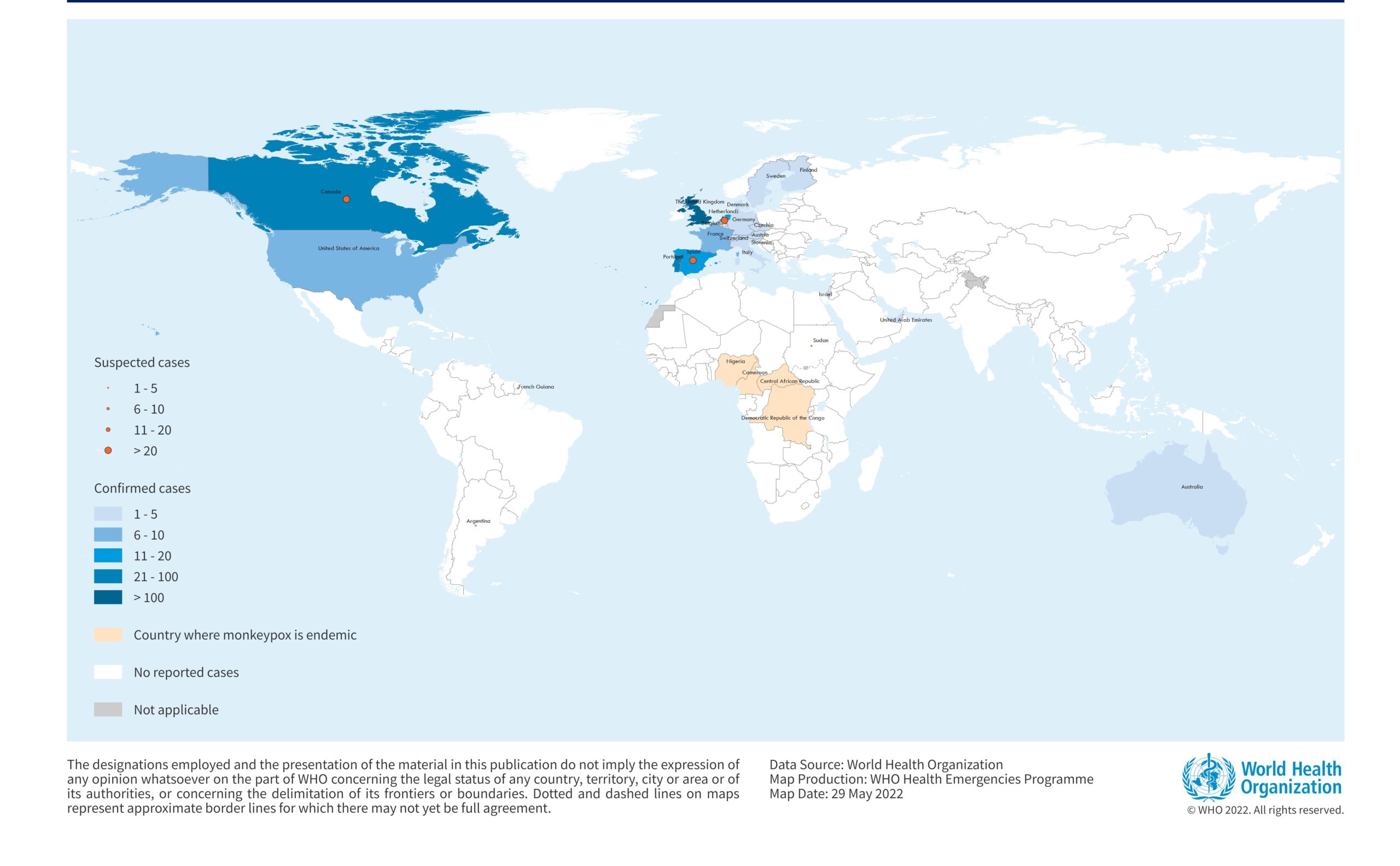
Since 13 May 2022, monkeypox has been reported to WHO from 23 Member States that are not endemic to the monkeypox virus, across four WHO regions. Epidemiological investigations are ongoing. The vast majority of reported cases so far have no established travel links to an endemic area and have presented through primary care or sexual health services. The identification of confirmed and suspected cases of monkeypox with no direct travel links to an endemic area is atypical. Early epidemiology of initial cases notified to WHO by countries shows that cases have been mainly reported amongst men who have sex with men (MSM). One case of monkeypox in a non-endemic country is considered an outbreak. The sudden appearance of monkeypox simultaneously in several non-endemic countries suggests that there may have been undetected transmission for some time as well as recent amplifying events.
The current publication of Disease Outbreak News is an update to the previously published Disease Outbreak News of 21 May. This edition provides information on recently published WHO guidance for the outbreak. The background information, such as the description of the epidemiology of the disease, remains mostly unchanged.
Description of the outbreak
As of 26 May, a cumulative total of 257 laboratory confirmed cases and around 120 suspected cases have been reported to WHO. No deaths have been reported.
The situation is evolving rapidly and WHO expects that there will be more cases identified as surveillance expands in non-endemic countries, as well as in countries known to be endemic who have not recently been reporting cases.
Immediate actions should focus on the following:
- providing accurate information to those who may be most at risk of monkeypox.
- stopping further spread among groups at risk.
- protecting frontline health workers.
Table 1. Cases of monkeypox in non-endemic countries to WHO between 13 May to 26 May 2022, 5 PM CEST

In addition to non-endemic countries reporting cases, WHO continues to receive updates on the status of ongoing outbreaks through established surveillance mechanisms (IDSR) for cases in endemic countries 1 in the African region. Laboratory strengthening in endemic countries is a priority to enable confirmation of suspected cases.
Table 2. Cases of monkeypox in endemic countries

For additional information please refer to WHO AFRO Weekly Bulletin on Outbreaks and Other Emergencies.
Figure 1. Geographical distribution of confirmed and suspected cases of monkeypox in non-endemic countries between 13 to 26 May 2022, 5 PM CEST.

Epidemiology of the disease
Monkeypox is a viral zoonosis (a virus transmitted to humans from animals) with symptoms very similar to those seen in the past in smallpox patients, although it is clinically less severe. It is caused by the monkeypox virus which belongs to the Orthopoxvirus genus of the Poxviridae family. The name monkeypox originates from the initial discovery of the virus in monkeys in Statens Serum Institute, Copenhagen Denmark, in 1958. The first human case was identified in a young child in the Democratic Republic of the Congo in 1970.
Monkeypox virus is transmitted from one person to another by close contact with lesions, body fluids, respiratory droplets and contaminated materials such as bedding. The incubation period of monkeypox is usually from 6 to 13 days but can range from 5 to 21 days.
Various animal species have been identified as susceptible to the monkeypox virus. Uncertainty remains on the natural history of the monkeypox virus and further studies are needed to identify the reservoir(s) and how virus circulation is maintained in nature. Eating inadequately cooked meat and other animal products of infected animals is a possible risk factor.
Monkeypox is usually self-limiting but there is likely to be little immunity to monkeypox among people living in non-endemic countries since the virus has not previously been identified in those populations. There are two clades of monkeypox virus: the West African clade and the Congo Basin (Central African) clade. The Congo Basin clade appears to cause severe disease more frequently with case fatality ratio (CFR) previously reported of up to around 10%. Currently, the Democratic Republic of the Congo is reporting a CFR among suspected cases of around 3%. The West African clade has in the past been associated with an overall lower CFR of around 1% in a generally younger population in the African setting. Since 2017, the few deaths of persons with monkeypox in West Africa have been associated with young age or an untreated HIV infection.
Historically, vaccination against smallpox had been shown to be cross-protective against monkeypox. However, immunity from smallpox vaccination will be limited to older persons since populations worldwide under the age of 40 or 50 years no longer benefit from the protection afforded by prior smallpox vaccination programmes. In addition, protection may have waned over time since vaccination.
While one smallpox vaccine (MVA-BN) and one specific treatment (tecovirimat) were approved for monkeypox in different countries, in 2019 and 2022 respectively, these countermeasures are not yet widely available in most countries and not at all in some.
Public health response
- Public health outbreak investigations are ongoing in countries that have identified cases, including extensive case finding and contact tracing, laboratory investigation, clinical management and case isolation. This is the approach WHO recommends to contain further spread.
- Diagnostic assays specific for monkeypox such as polymerase chain reaction (PCR) assays have so far found that the West Africa clade of the monkeypox virus is present in this multi-country outbreak. Genomic sequencing, where available, is being undertaken to further characterize the monkeypox virus circulating in this outbreak. Several European countries (Belgium, France, Germany, the Netherlands, and Portugal) have published full-length or draft genome sequences of the monkeypox virus for the current outbreak. While investigations are ongoing, preliminary data confirm that the genomes belong to the West African clade of monkeypox virus.
- Smallpox and monkeypox vaccines, where available, are being deployed in a limited number of countries to manage close contacts. While smallpox vaccines have been shown to be protective against monkeypox, there is also one vaccine approved for prevention of monkeypox. This vaccine is based on a strain of vaccinia virus (known generically as modified vaccinia Ankara Bavarian Nordic strain, or MVA-BN). This vaccine has been approved for prevention of monkeypox in Canada and the United States of America. In the European Union, this vaccine has been approved for prevention of smallpox. WHO has convened experts to review the latest data on smallpox and monkeypox vaccines, and to provide guidance on how and in what circumstances they should be used.
- WHO has published rapid interim guidance on:
- Surveillance, case investigation and contact tracing for monkeypox to rapidly identify cases and clusters in order to provide optimal clinical care; to isolate cases to prevent further transmission; to identify and manage close contacts; to protect frontline health workers; and to tailor effective control and prevention measures. This interim guidance includes case definitions.
- Laboratory testing for the monkeypox virus to enable timely and accurate confirmation of infection, to support outbreak investigations and the breaking of chains of transmission, and to control and stop the outbreak
- Monkeypox: public health advice for gay, bisexual and MSM is provided to support development of risk communication and community engagement messages for persons at higher risk in the early stages of this outbreak.
WHO interim guidance for health authorities on the clinical management of monkeypox and infection prevention and control (IPC), vaccines and immunization for monkeypox, and risk communication and community engagement will be published shortly.
WHO risk assessment
Currently, the overall public health risk at global level is assessed as moderate considering this is the first time that monkeypox cases and clusters are reported concurrently in widely disparate WHO geographical areas, and without known epidemiological links to non-endemic countries in West or Central Africa. Cases have been mainly reported amongst MSM. Additionally, the sudden appearance and wide geographic scope of many sporadic cases indicates that widespread human-to-human transmission is already underway, and the virus may have been circulating unrecognized for several weeks or longer.
The public health risk could become high if this virus exploits the opportunity to establish itself as a human pathogen and spreads to groups at higher risk of severe disease such as young children and immunosuppressed persons; a large part of the population is vulnerable to monkeypox virus, as smallpox vaccination, which confers some cross-protection, has been discontinued since 1980 or earlier in some countries.
There is currently limited epidemiological and laboratory information, and the number of cases currently being reported is likely to be an underestimate, in part due the following:
- the relatively mild symptoms in many cases with localized rash and lymphadenopathy, such that many persons may not present to health care services
- lack of early clinical recognition by health workers of an infection previously known in only a few countries;
- the time required by Member States to establish and scale up new surveillance mechanisms.
- and a lack of widely available diagnostic tests, reagents and other supplies.
There is a potential risk to health workers if they are not wearing appropriate personal protective equipment (PPE) to prevent transmission. Though not reported in the current outbreak, the risk of health care associated monkeypox infections has been documented in the past.
There is the potential for greater health impact with wider spread to vulnerable population groups, as deaths among cases in previous outbreaks have been reported to occur more often among children, and immunocompromised individuals, including persons with poorly controlled HIV infection, who may be especially at risk of more severe disease.
Furthermore, there is the high likelihood of identification of further cases with unidentified chains of transmission, including potentially in other population groups. With a number of countries in several WHO regions reporting cases of monkeypox, it is highly likely that even more countries will identify cases. As monkeypox lesions commonly occur on the skin over many or all parts of the body, as well as in the mouth, there is a high risk of further spread of the virus through close physical contact within families or with sexual partners, including face-to-face, skin-to-skin, or mouth-to-skin contact, or contact with contaminated materials (e.g., linen, bedding, clothing or utensils). However, at present, the risk for the general public appears to be low. Nonetheless, immediate action from countries is required to control further spread among groups at risk, prevent spread to the general population and avert the establishment of monkeypox as a clinical condition and public health problem in currently non-endemic countries.
WHO advice
Identification of additional cases and further onward spread in currently affected and other Member States is likely. Countries should be on the alert for signals related to patients presenting with a rash that progresses in sequential stages – macules, papules, vesicles, pustules, scabs, at the same stage of development over all affected areas of the body – that may be associated with fever, enlarged lymph nodes, headache, back pain, muscle aches or fatigue. During this current outbreak, many individuals are presenting with localized rash – oral, peri-genital and/or peri-anal distribution associated with painful regional lymphadenopathy – sometimes with secondary infection. These individuals may present to various community and health care settings including but not limited to primary care, fever clinics, sexual health services, travel health clinics, infectious disease units, emergency departments, dermatology clinics, obstetrics and gynaecology, and dental services. Increasing awareness among potentially affected communities, as well as health care providers and laboratory workers, is essential for identifying and preventing further secondary cases and effective management of the current outbreak.
Any individual meeting the definition for a suspected case should be offered testing. The decision to test should be based on both clinical and epidemiological factors, linked to an assessment of the likelihood of infection. Due to the range of conditions that cause skin rashes and because clinical presentation may more often be atypical in this outbreak, it can be challenging to differentiate monkeypox solely based on the clinical presentation, particularly for cases with an atypical presentation. Any patient with suspected monkeypox should be investigated and if confirmed, isolated until their lesions have crusted, the scab has fallen off and a fresh layer of skin has formed underneath. Isolation can occur either in a health care facility or at home, provided the infected individual can be isolated and cared for appropriately. All efforts should be made to avoid unnecessary stigmatization of individuals and communities potentially affected by monkeypox.
Considerations relating to surveillance and reporting
For further details please refer to; WHO Surveillance, case investigation and contact tracing for Monkeypox: Interim guidance, 22 May 2022.
Surveillance
The key objectives of surveillance and case investigation for monkeypox in the current context are to rapidly identify cases and clusters of infection and the sources of infection as soon as possible in order to provide clinical care and isolate cases to prevent further transmission; and to tailor effective control and prevention measures based on most commonly identified routes of transmission. In non-endemic countries, one case is considered an outbreak. Because of the public health risks associated with a single case of monkeypox, clinicians should report suspected cases immediately to their local or national public health authorities according to national reporting protocols, regardless of whether they are also exploring other potential diagnoses. Cases should be reported immediately, according to the case definitions (link shared above, under public health response) or nationally tailored case definitions. Probable and confirmed cases should be reported immediately to WHO through IHR national focal points (NFPs) under the International Health Regulations (IHR 2005).
Countries should be on the alert for signals related to patients presenting with unusual rash, vesicular or pustular lesions or lymphadenopathy, often associated with fever, in a range of community and health care settings, including but not limited to primary care, fever clinics, sexual health services, travel health clinics, infectious disease units, emergency services, obstetrics and gynaecology, and dermatology clinics. Surveillance for rash-like illness should be intensified and guidance provided for collection of skin lesion samples for confirmatory PCR testing. Clinicians should be on the alert for any patient with relevant symptoms and signs who may have recently travelled or been in contact with someone who has recently travelled. This includes but is not limited to travel from endemic countries, and particularly Nigeria at this time, or travel from other countries where monkeypox has recently been reported. Persons who have recently had close personal contact with multiple sexual partners, whether locally or in connection with recent travel, may be at risk. Outreach activities should be put in place for communities identified to be at risk as the outbreak unfolds. At the present time, this includes outreach to social networks of MSM and their close contacts. It is important to note that the first case of monkeypox identified in any community may have acquired infection through close personal contact locally. In limited circumstances, recent preparation or consumption of wild game or bushmeat may also represent a risk.
Reporting
Case reports should include at a minimum the following information: date of report; reporting location; name, age, sex and residence of case; date of onset of first symptoms; recent travel history including location and dates of travel; recent exposure to a probable or confirmed case; relationship and nature of contact with probable or confirmed case (where relevant); recent history of multiple and/or anonymous sexual partners; smallpox or monkeypox vaccination status; presence of rash; presence of other clinical signs or symptoms as per case definition; clinical diagnosis and date of laboratory confirmation (where done); method of confirmation (where done); genomic characterization (if available); other relevant clinical or laboratory findings, particularly to exclude common causes of rash as per the case definition; whether hospitalized; date of hospitalization (where relevant); and outcome at time of reporting.
A global case reporting form is under development.
Considerations related to case investigation
Rationale
During human monkeypox outbreaks, close physical contact with infected persons is the most significant risk factor for monkeypox virus infection. If monkeypox is suspected, the investigation should consist of (i) clinical examination of the patient using appropriate infection prevention and control (IPC) measures, (ii) questioning the patient about possible local or travel-related sources of infection and the presence of similar disease in the patient’s community and contacts, and (iii) collection and dispatch of specimens for monkeypox laboratory examination. The minimum data to be captured are included above under ‘Reporting’. Exposure investigation should cover the period up to 21 days prior to symptom onset. Any patient with suspected monkeypox should be isolated during the presumed and known infectious periods, that is during the prodromal and rash stages of the illness, respectively. Laboratory confirmation of suspected cases is important but should not delay public health actions. Suspected presence of similar disease in the patient’s community or contacts should be further investigated (also known as “backwards contact tracing”).
Retrospective cases found by active search may no longer have the clinical symptoms of monkeypox (they have recovered from acute illness) but may exhibit scarring and other sequelae. It is important to collect epidemiological information from retrospective cases in addition to active ones.
Samples taken from people with suspected monkeypox or animals with suspected monkeypox virus infection should be safely handled by trained staff working in suitably equipped laboratories. National and international regulations on transport of infectious substances should be strictly followed during the sample packing and transportation to the testing laboratories. Careful planning is required to consider laboratory testing capacity. Clinical laboratories should be informed in advance of samples to be submitted from persons with suspected or confirmed monkeypox, so that they can minimize risk to laboratory workers and, where appropriate, safely perform laboratory tests that are essential for clinical care. See further information below: Considerations for laboratory testing and sample management.
Retrospective cases cannot be laboratory confirmed; however, serum from retrospective cases can be collected and tested for anti-orthopoxvirus antibodies to aid in their case classification.
Considerations related to contact tracing
Rationale
Contact tracing is a key public health measure to control the spread of infectious disease pathogens such as monkeypox virus. It allows for the interruption of transmission and can also help people at a higher risk of developing severe disease to more quickly identify their exposure, so that their health status can be monitored, and they can seek medical care more quickly if they become symptomatic. In the current context, as soon as a suspected case is identified, contact identification and contact tracing should be initiated. Case patients should be interviewed to elicit the names and contact information of all such persons. Contacts should be notified within 24 hours of identification.
Definition of a contact
A contact is defined as a person who, in the period beginning with the onset of the source case’s first symptoms, and ending when all scabs have fallen off, has had one or more of the following exposures with a probable or confirmed case of monkeypox:
- direct physical or intimate personal contact, including any sexual contact
- face-to-face exposure (including health workers without appropriate PPE)
- contact with contaminated materials such as clothing or bedding
Contact identification
Case-patients can be prompted to identify contacts across different contexts, including their household, intimate partners and sexual contacts, as well as events and social gatherings where extended networks of individuals may engage in activities involving physical contact that may put participants at risk, festivals, sports, bars or restaurants and other gathering places, transportation or travel in a closed vehicle, health care (including laboratory exposure), the workplace, houses of worship, school/nursery, and any other recalled interactions. Attendance lists and, passenger manifests, for example, can be further used to identify contacts.
Contact monitoring
Contacts should be monitored at least daily for the onset of signs/symptoms for a period of 21 days from last contact with a patient in the infectious period. Signs/symptoms of concern include feeling unwell, headache, fever, chills, sore mouth or throat, malaise, fatigue, rash, and lymphadenopathy (swollen or inflamed lymph nodes). Contacts should monitor their temperature twice daily. Contacts without any symptoms should not donate blood, cells, tissue, organs, breast milk, or semen while they are self-monitoring or being monitored for symptoms. Contacts without symptoms can continue routine daily activities such as going to work and attending school (i.e., no quarantine is necessary), but should remain close to home for the duration of the period of monitoring. It may, however, be prudent to exclude pre-school children from day care, nursery or other group settings.
Options for monitoring by public health authorities are dependent on available resources. Contacts can self-monitor or be monitored actively, or directly. For self-monitoring, identified contacts are provided with information on the signs/symptoms to monitor, permitted activities, and how to contact the public health department if signs/symptoms develop. Active monitoring is when public health officials are responsible for checking at least once a day to see if a person under monitoring has self-reported signs/symptoms. Direct monitoring is a variation of active monitoring that involves at least daily home visiting or attendance at a health facility or public health unit if this can be done safely, or visually examining the person under monitoring via video for signs of illness.
A contact who develops initial signs/symptoms other than rash should be isolated and closely watched for signs of rash for the next seven days. If no rash develops, the contact can return to temperature monitoring for the remainder of the 21 days. If the contact develops a rash, they must be isolated or self-isolate as appropriate, they must be fully evaluated as a suspected case, and a specimen should be collected for laboratory analysis to test for monkeypox.
Monitoring exposed health workers and caregivers
Any health worker or household member who has cared for a person with probable or confirmed monkeypox, including management of potentially contaminated materials even without direct patient contact, should be alert to the development of symptoms that could suggest acquisition of monkeypox infection, especially within the 21-day period after the last date that care was provided. Health workers should notify infection control, occupational health, and public health authorities to be guided about a medical evaluation.
Health workers who have unprotected exposures (i.e., not wearing appropriate PPE) to patients with monkeypox or contact with possibly contaminated materials do not need to be excluded from work duty if they are without symptoms during the monitoring period but should undergo monitoring for symptoms, which includes measurement of temperature at least twice daily for 21 days following the exposure. Prior to reporting for work each day, the health worker should be interviewed regarding evidence of any relevant signs/symptoms as above.
Health workers who have cared for or otherwise been in direct or indirect contact with monkeypox patients while adhering to recommended infection control precautions may undergo self-monitoring or active monitoring as determined by local public health authorities.
Vaccination of contacts and /or health personnel
Some countries may hold monkeypox or smallpox vaccine which could be considered for use according to national guidance. Where feasible, countries could consider timely vaccination of close contacts as post-exposure prophylaxis. Post-exposure vaccination with locally available monkeypox or smallpox vaccine (ideally within 4 days of exposure) may be considered by some countries for higher risk contacts, such as family living in the same household, intimate personal or sexual contacts, or health workers exposed while not wearing appropriate PPE. Decisions on vaccination and which vaccine to use should be based on national guidance. Individual decisions on vaccination for contacts of patients with monkeypox should be based on public health guidance, risk-benefit assessment and shared clinical decision-making between a health care provider and a patient contact. Pre-exposure vaccination may also be considered for certain health workers, including laboratory personnel, or other persons at risk.
Any request for vaccines should be directed through health authorities at national level.
Travel-related contact tracing
Public health officials should work with travel operators and public health counterparts in other locations to assess potential risks and to contact passengers or others who may have had contact with an infectious patient while in transit.
A global contact tracing form will be made available shortly.
Considerations related to risk communication and community engagement
Communicating monkeypox related risks and engaging with at-risk and affected communities, civil society organizations, and health care providers, including sexual health clinics, on prevention, detection and care, is essential for preventing further secondary cases and effective management of the current outbreak. Providing public health advice on how the disease transmits, its symptoms and preventive measures and targeting community engagement to the population groups who are most at risk, is critical to minimize spread.
Anyone who has direct contact with an infected person, including intimate or sexual contact can get monkeypox. Steps for self-protection include avoiding physical contact with the person. It is also critical to avoid intimate or sexual contact with someone with a localized anogenital rash and/or oral ulcers. During the early phase of this outbreak while information is still being collected, it would be prudent to limit the number of sex partners, keep hands clean with water and soap or alcohol-based gels, and maintain respiratory etiquette and hand hygiene.
If people develop a rash, accompanied by fever or a feeling of discomfort or illness, they should contact their health care provider and get tested for monkeypox. If someone is suspected or confirmed as having monkeypox, they should isolate at home or in an appropriate facility until the scabs have fallen off, and abstain from sex, including oral sex. During this period, patients must be offered supportive medical care to ease monkeypox symptoms such as pain or itchiness. Patients should be monitored for early detection of any medical complications of the illness. Anyone caring for a person sick with monkeypox should use appropriate personal protective measures.
Any rash-like illness during travel or upon return should be immediately reported to a health professional, including information about all recent travel, sexual history and smallpox immunization history.
Residents and travelers to monkeypox-endemic countries should avoid contact with sick mammals such as rodents, marsupials, non-human primates (dead or alive) that could harbour monkeypox virus and should refrain from eating or handling wild game (bush meat).
Considerations related to clinical management and infection prevention and control in health care settings
These precautions are applicable in any health facility including outpatient services and hospitals.
Health workers caring for patients with suspected or confirmed monkeypox should implement standard, contact and droplet precautions. These precautions are applicable in any health facility including outpatient services and hospitals. Standard precautions include strict adherence to hand hygiene, appropriate handling of contaminated medical equipment, laundry, waste and cleaning and disinfection of environmental surfaces
WHO advises that contact and droplet transmission-based precautions be implemented at a minimum for any suspected or confirmed case of monkeypox. This includes:
- All health workers should perform hand hygiene according to the WHO 5 moments of hand hygiene, including prior to putting on and after removing PPE.
- Place patient in a well-ventilated single patient room with dedicated bathroom or toilet. If single patient rooms are not available, consider cohorting confirmed cases, maintaining a distance of 1-metre between patients.
- Designated patient room/area should have signage posted at the entrance indicating contact/droplet precautions.
- Anyone entering the patient room should wear personal protective equipment (PPE) including gloves, gown, a well-fitting medical mask and eye protection
- Instruct the patient to wear a well-fitting medical mask and follow respiratory hygiene and cough etiquette and cover exposed lesions when others are in the room and when transport is necessary.
- Avoid unnecessary movement of persons with suspected or /confirmed monkeypox. If the patient must be moved or transported within or beyond the facility, ensure risk-based precautions are maintained, and place a well-fitting medical mask on the patient (provided the patient is able to tolerate).
- The receiving facility/ward/unit should be aware of transmission-based precautions required in order to inform the staff and prepare the isolation or designated area.
- Should any aerosol-generating procedures be required for patient care and cannot be deferred, health workers should take all the necessary precautions to avoid aerosolization of patient secretions or other material and don the appropriate PPE necessary to protect themselves during the procedure.
PPE should be disposed of prior to leaving the isolation area where the patient is admitted. Areas within the health care facility frequently used by the patient or where patient care activities occur, and patient care equipment should be cleaned and disinfected as per national or facility guidelines. Linens, hospital gowns, towels and any other fabric items should be handled and collected carefully to avoid shaking.
Full interim guidance on infection prevention and control will be published shortly.
Clinical management and treatment
Clinical care for patients with monkeypox is supportive. All symptoms should be attended to including fever, painful sores or skin lesions, discomfort related to swollen lymph nodes or any other concerns. Patients should have plenty of rest and fluids, as systemic symptoms (e.g., fever) may lead to dehydration and localized symptoms (e.g., sores in the mouth or swollen lymph nodes) may result in difficulty eating or drinking enough liquids. Care should be taken to avoid touching mucous membranes such as the eyes and secondary infections of lesions must be prevented or treated according to local medical protocols. Proper eye and skin care will help to reduce complications and sequelae such as scarring. Patients should also be monitored to ensure that swelling of lymph nodes or abscesses in the mouth or throat do not compromise the ability to breath or lead to respiratory obstruction. All underlying conditions or associated infections due to other causes should be promptly and fully treated.
Deployment of pharmaceutical countermeasures including specific antivirals (i.e., tecovirimat, which is approved for monkeypox, but not yet widely available) can be considered under investigational or compassionate use protocols particularly for those who have severe symptoms or who may be at risk of poor outcomes (such as those with immune suppression due to other medical conditions or young children).
Full interim guidance on clinical care and therapeutics for monkeypox will be published shortly.
Considerations related to laboratory testing and sample management
For more details, please refer to WHO Laboratory testing for the monkeypox virus: Interim guidance, 23 May 2022.
Monkeypox virus (MPXV) is a double-stranded DNA virus, a member of the Orthopoxvirus genus within the Poxviridae family. Poxviruses cause disease in humans and many other animals; infection typically results in the formation of lesions, skin nodules or disseminated rash. Other orthopoxvirus (OPXV) species pathogenic to humans include cowpox virus, and variola virus (causing smallpox, which has been eradicated). Vaccinia virus is also an OPXV that has been used to produce vaccines for immunizing people and was a key tool for the eradication of smallpox, achieved in 1980.
The recommended specimen type for laboratory confirmation of monkeypox is skin lesion material, including swabs of lesion surface and/or exudate, roofs from more than one lesion, or lesion crusts. Alternatively, swabs placed in viral transport media (VTM) can also be used. Specimens should be stored refrigerated or frozen within an hour of collection and transported to the laboratory as soon as possible after collection. If transport exceeds seven days for the sample to be tested, specimens should be stored at -20 celsius or lower.
All specimens being transported should have appropriate triple packaging, labelling and documentation and be shipped in compliance with applicable national and/or international regulations. Shipping requires a dangerous goods certified shipper. For information on infectious substances shipping requirements, please see the WHO Guidance on regulations for the transport of infectious substances 2021-2022.
Confirmation of monkeypox infection is based on nucleic acid amplification testing (NAAT), using real-time or conventional PCR, for detection of unique sequences of MPXV viral DNA. If a MPXV specific test (preferable) is not available, an orthopoxvirus positive PCR can be considered confirmation in non-endemic countries, as there is little circulation of other orthopoxviruses in humans. PCR can be used alone, or in combination with sequencing.
Antibody detection from plasma or serum should not be used alone for diagnosis of monkeypox. However, IgM detection from recent acutely ill patients or IgG in paired serum samples, collected at least 21 days apart, with the first being collected during the first week of illness, can aid diagnosis if tested samples yield inconclusive results. Recent or previous smallpox vaccination may interfere with serological testing.
Electron microscopy can be used to visualize potential poxvirus in the sample, but with the availability of molecular assays and the high technical skills and facility required, this method is not routinely used for laboratory confirmation.
Virus isolation is not recommended as a routine diagnostic procedure and should only be performed in laboratories with appropriate experience and containment facilities. Confirmation of monkeypox infection should consider clinical and epidemiological information. All test results, positive or negative, should be immediately reported to national authorities. Access to timely and accurate laboratory testing of samples from cases under investigation is an essential part of the diagnosis and surveillance of this emerging infection. All countries should have access to reliable testing either nationally or through referral to laboratories in other countries that are willing and able to undertake OPXV or MPXV detection. WHO, through its Regional Offices, can assist Member States to access testing through referral. Countries are encouraged to undertake and share their sequence data through publicly accessible databases for a better understanding of the epidemiology and monkeypox evolution in the current outbreak.
Based on available information at this time, WHO does not recommend that Member States adopt any international travel-related measure for either incoming or outgoing travelers.
WHO will be providing additional interim guidance on case management and infection, prevention and control; vaccines and immunization, and risk communication and community engagement in the coming days.
WHO urges all Member States, health authorities at all levels, clinicians, health and social sector partners, and academic, research and commercial partners to respond quickly to stop the multi-country outbreak of monkeypox. Rapid action must be taken before the virus can be allowed to establish itself as a human pathogen with efficient person-to-person transmission in both endemic and non-endemic contexts. Lessons learned from the eradication of smallpox and from the management of other emerging zoonotic diseases must be urgently considered in the light of these rapidly evolving events.







{kind=link}