

Clinicians are well aware of the benefits of physical activity — and the consequences of inactivity.
Managing the diseases associated with inactivity — heart disease, type 2 diabetes, hypertension — falls to physicians. So one might assume they routinely prescribe exercise to their patients, just as they would statins, insulin, or beta-blockers.
But evidence indicates doctors don’t routinely have those conversations. They may lack confidence in their ability to give effective advice, fear offending patients, or simply not know what to say.
That’s understandable. Many doctors receive little training on how to counsel patients to exercise, according to research over the past decade. Despite efforts to improve this, many medical students still feel unprepared to prescribe physical activity to patients.
But here’s the thing: Doctors are in a unique position to change things.
Only 28% of Americans meet physical activity guidelines, according to the Centers for Disease Control and Prevention. At the same time, other research suggests that patients want to be more active and would like help from their doctor.
“Patients are motivated to hear about physical activity from physicians and try to make a change,” says Jane Thornton, MD, PhD, an assistant professor in family medicine at Western University in Ontario, Canada. “Just saying something, even if you don’t have specialized knowledge, makes a difference because of the credibility we have as physicians.”
Conveniently, just like exercise, the best way to get started is to…get started.
Here’s how to break down the process into steps.
1. Ask patients about their physical activity.
Think of this as taking any kind of patient history, only for physical activity.
Do they have a regular exercise routine? For how many minutes a day are they active? How many days a week?
“It takes less than a minute to ask and record,” Thornton says. Once you put it into the patient’s electronic record, you have something you can track.
2. Write an actual prescription .
By giving the patient a written, printed prescription when they leave your office, “you’re showing it’s an important part of treatment or prevention,” Thornton explains. It puts physical activity on the level of a vital sign.
Include frequency, intensity, time, and type of exercise. The American College of Sports Medicine’s Exercise is Medicine initiative provides a prescription template you can use.
3. Measure what they do.
Measurement helps the patient adopt the new behavior, and it helps the physician provide tailored advice going forward, Thornton says.
With the rise of health-monitoring wearables, tracking activity has never been easier. Of course, not everyone wants to (or can afford to) use a smartwatch or fitness tracker.
For tech-averse patients, ask if they’re willing to write something down, like how many minutes they spent walking, or how many yoga classes they attended. You may never get this from some patients, but it never hurts to ask.
4. Refer out when necessary.
This brings us to a sticky issue for many physicians: lack of confidence in their ability to speak authoritatively about physical activity. “In most cases, you can absolutely say, ‘Start slow, go gradually,’ that kind of thing,” Thornton says. “As with anything, confidence will come with practice.”
For specific prescriptive advice, check out the Exercise is Medicine website, which also has handouts you can share with patients and information for specific conditions. If your patient has prediabetes, you can also point them toward the CDC’s diabetes prevention program, which is available in-person or online and may be free or covered by insurance.
If a patient has contraindications, refer out. If you don’t have exercise or rehab professionals in your network, Thornton recommends reaching out to your regional or national association of sports-medicine professionals. You should be able to find it with a quick Google search.
5. Follow up.
Ask about physical activity during every contact, either in person or online.
Thornton says the second and fifth steps matter most to patients, especially when the prescription and follow-up come from their primary care physician, rather than a nurse or physician assistant to whom you’ve delegated the task.
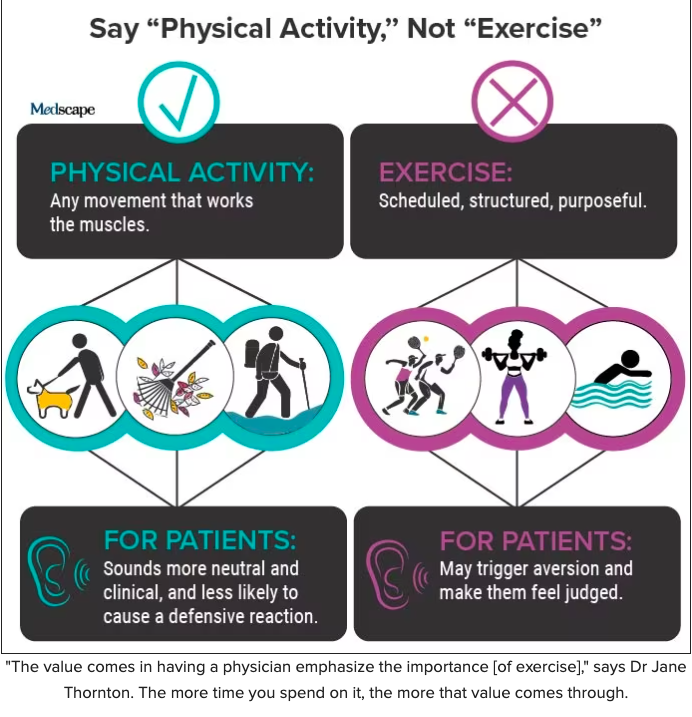
“The value comes in having a physician emphasize the importance,” Thornton says. The more time you spend on it, the more that value comes through.
What NOT to Say to Patients About Exercise
This might surprise you:
“I definitely don’t think telling people the official recommendations for physical activity is useful,” says Yoni Freedhoff, MD, an associate professor of family medicine at the University of Ottawa and medical director of the Bariatric Medical Institute. “If anything, I’d venture it’s counterproductive.”
It’s not that there’s anything wrong with the recommended minimum — 150 minutes of moderate-to-vigorous-intensity physical activity per week. The problem is what it says to a patient who doesn’t come close to those standards.
“Few real-world people have the interest, time, energy, or privilege to achieve them,” Freedhoff says. “Many will recognize that instantly and consequently feel less than that is pointless.”
And that, Thornton says, is categorically not true. “Even minimal physical activity, in some cases, is beneficial.”
You also want to avoid any explicit connection between exercise and weight loss, Thornton says.
Though many people do connect the two, the link is often negative, notes a 2019 study from the University of Toronto, triggering painful memories that might go all the way back to gym class.
Try this pivot from Freedhoff: “Focus on the role of exercise in mitigating the risks of weight,” he says — like decreasing pain, increasing energy, and improving sleep.
How to Motivate Patients to Move
New research backs up this more positive approach. In a study published today in Annals of Internal Medicine, doctors in the UK who emphasized benefits and minimized health harms convinced more patients to join a weight management program than negative or neutral docs did. These doctors conveyed optimism and excitement, smiling and avoiding any mention of obesity or body mass index.
Exactly what benefits inspire change will be different for each patient. But in general, the more immediate the benefit, the more motivating it will be.
As the University of Toronto study noted, patients weren’t motivated by vague, distant goals like “increasing life expectancy or avoiding health problems many years in the future.”
They’re much more likely to take action to avoid surgery, reduce medications, or minimize the risk of falling.
For an older patient, Freedhoff says, “focusing on the preservation of functional independence can be extremely motivating.” That’s especially true if the patient has vivid memories of seeing a sedentary loved one decline late in life.
For patients who may be more focused on appearance, they could respond to the idea of improving their body composition. For that, “we talk about the quality of weight loss,” says Spencer Nadolsky, DO, an obesity and lipid specialist and medical director of WeightWatchers. “Ultimately, exercise helps shape the body instead of just changing the number on the scale.”
Reducing Resistance to Resistance Training
A conversation about reshaping the body or avoiding age-related disabilities leads naturally to resistance training.
“I always frame resistance training as the single most valuable thing a person might do to try to preserve their functional independence,” Freedhoff says. If the patient is over 65, he won’t wait for them to show an interest. “I’ll absolutely bring it up with them directly.”
Freedhoff has an on-site training facility where trainers show patients how to work out at home with minimal equipment, like dumbbells and resistance bands.
Most doctors, however, don’t have those options. That can lead to a tricky conversation. Participants in the University of Toronto study told the authors they disliked the gym, finding it “boring, intimidating, or discouraging.”
And yet, “a common suggestion…from healthcare providers was to join a gym.”
Many patients, Nadolsky says, associate strength training with “grunting, groaning, or getting ‘bulky’ vs. ‘toned.’ ” Memories of soreness from overzealous workouts are another barrier.
He recommends “starting small and slow,” with one or two full-body workouts a week. Those initial workouts might include just one to two sets of four to five exercises. “Consider if someone is exercising at home or in a gym to build a routine around equipment that’s available to them,” Nadolsky says.
Once you determine what you have to work with, help the patient choose exercises that fit their needs, goals, preferences, limitations, and prior injuries.
One more consideration: While Nadolsky tries to “stay away from telling a patient they need to do specific types of exercise to be successful,” he makes an exception for patients who’re taking a GLP-1 agonist. “There is a concern for muscle mass loss along with fat loss.”
Practicing, Preaching, and Checking Privilege
When Thornton, Freedhoff, and Nadolsky discuss exercise, their patients know they practice what they preach.
Nadolsky, who was a nationally ranked wrestler at the University of North Carolina, hosts the Docs Who Lift podcast with his brother, Karl Nadolsky, MD.
Freedhoff is also a lifter and fitness enthusiast.
And Thornton was a world-class rower whose team came within 0.8 seconds of a silver medal at the Beijing Olympics. (They finished fourth.)
But not all physicians follow their own lifestyle advice, Freedhoff says. That doesn’t make them bad doctors — it makes them human.
“I’ve done 300 minutes a week of exercise” — the recommended amount for weight maintenance — “to see what’s involved,” Freedhoff says. “That’s far, far, far from a trivial amount.”
That leads to this advice for his fellow physicians:
“The most important thing to know about exercise is that finding the time and having the health to do so is a privilege,” he says.
Understanding that is crucial for assessing your patient’s needs and providing the right help.
Source: Medscape









{kind=link}